


How Does the HUB Get Missed? What are the Implications?
Shattering the Efficacy Illusion, Part 5

"If one harbors anywhere in one's mind a nationalistic loyalty or hatred, certain facts, though in a sense known to be true, are inadmissible." -George Orwell
Articles from the Vaccine Wars can be found here. See Part 1, Part 2, Part 3, and Part 4 if you're just getting started. This may be necessary to handle all the acronyms. My apologies for taking this series on a bit slowly. My attention has been pulled in many directions.
Why hasn't almost anyone (aside from a small handful of people) been talking about the HUB since the mass experimental quasi-vaccine rollout? Are we all hypnotized by the constant stream of shocking news? Are there just so many problems to focus on, and people trying to steer each of us away from a full examination of the Bigger Picture (I feel that pressure often), that an obvious point like this that has even been discussed in the past…escapes us? Or perhaps some clever coup is upon us?
Obligatory reminder: at the county level, all apparent (mild) vaccine effectiveness is entirely explained by the Healthy User Bias (HUB).
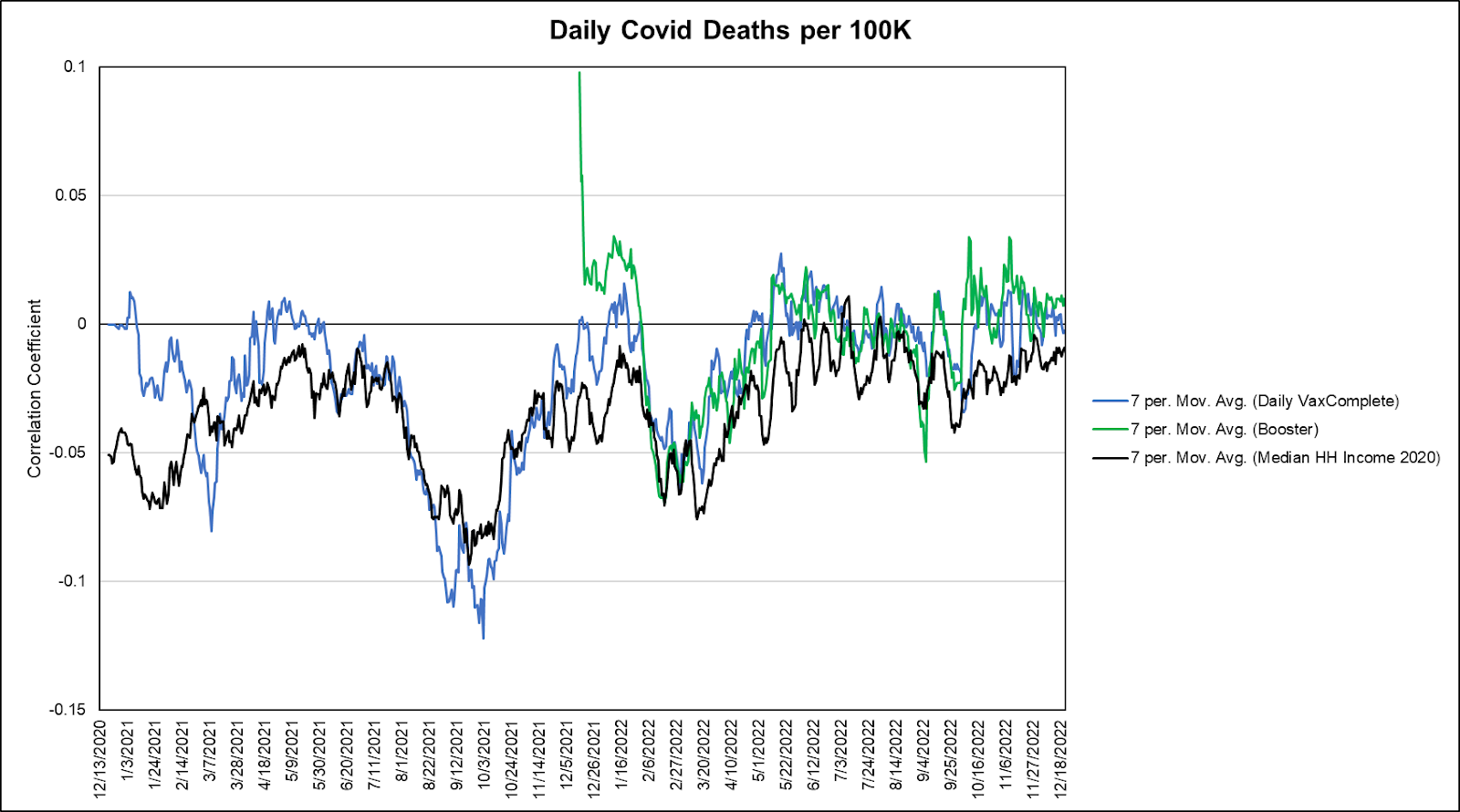
How Does the HUB Get Missed?
Let us understand first that the HUB is not even a concept on the tips of the tongues or minds of many of us who have been employed in Statistics work outside of the medical field. It may also be the case that those who are familiar with the concept have not explored it well enough to have intuition about its presence. Add to that the conflict of interests associated with the biomedical field, and you have the makings of a memory hole.
Aside from the true experts in the Statistics that can be applied to health related fields are the pseudo-experts: people trained to just the right level where they believe themselves to be experts. Professionalization of peak Dunning-Kruger. Just enough education to be dangerous, and certainly not enough to be enlightened to key concepts that distinguish science from a hall of mirrors. Above the dangerous folks sit gatekeepers of the system that sucks in public money into a political positive-feedback loop.

To be clear: Holden Thorp isn't just some guy with an opinion on the internet. He is the Editor-in-Chief of Science, and a former provost at my old university, which was the hub of the Human Genome Project. He was also the chancellor at the University of North Carolina at Chapel Hill, where Ralph Baric does his thing.

Despite all of the money poured into public health and data science, most all of the people capable of doing the job (of recognizing the HUB, and applying themselves to solve the problem) are either compromised (bribed, scared silent, or ideologically driven) or work elsewhere (like Big Tech where they can lounge in bean bag chairs eating soft-serve ice cream while earning enormous salaries for their part in helping to tear apart the fabric of society, or Wall Street where they are given tacit or explicit permission to abuse whomever they can).



Somehow I doubt that the surgeon general just tweeted his delight of eating empty carbohydrates.
Do you think he could be laughing about the vacuousness of vaccine effectiveness in that tweet?
My wife is an Instructor of Bioinformatics at a research university, but way back when she started her graduate work, she landed in an Epidemiology class more suited for teaching Woke political theory than helping anyone climb the ladder of understanding Statistics. In order to challenge herself to take the serious Calculus-based Statistics class during her PhD work, she spent 60 hours in my classroom where we rebuilt her basics to the point that she could solve all the problems and earn an A [in the Statistics course that matters in opening the door for real world work] with the solid base to move forward with, and expand on. Many people in that situation are not even aware of the gap between their foundation and rigorous mathematics. Even worse, the educational system is designed not to push most of those people to build a new foundation—but rather to play pretend. "Sure, your ability to plug these numbers into a calculator that spits out a number is what you need to be an expert in your field. Here's a pile of money for your troubles."
Also, the fact of the matter is that we have reached the point in the co-evolution of science alongside politics that, for the majority of young people entering the biohealth space, it pays to focus more on the politics than on the harder, rigorous stuff.
If there are ten primary stories about how modern science died, that's one of them.
What Would Effectiveness Look Like?
And what would ineffectiveness look like?
And which Epidemiologists would even know?
Try to ignore the red trend lines in the plots below. The one on the left was based on real world data (late 2021, but far enough into the vaccine rollout to be robust) and seemed to show a mild negative trend in COVID-19 deaths. The other four are random simulations based on an assumption of 95% efficacy. To most people, the differences in these plots are subtle. To a well-trained data mind, they are obviously vast.
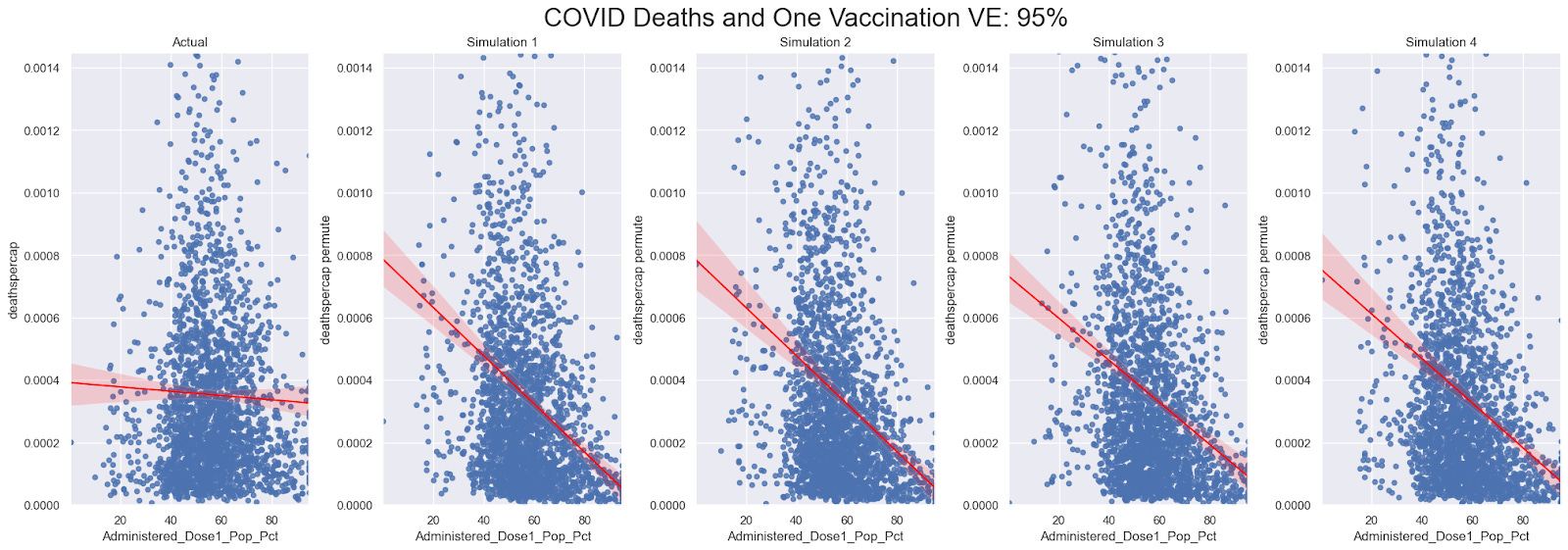
The only thing that's easy to understand is the trend line. In these representations of probabilistic and chaotic randomness, those trend lines tell us the degree of effectiveness of the COVID-19 vaccines in reducing mortality due to COVID-19. As we can see, there is barely any. As with the other four simulations, the trend line should be steep and unmistakable. And as we've seen in prior articles, that bit seems almost certainly based on identifiable differences between the vaccinated and unvaccinated cohorts.
Even correcting for the pitfalls at the educational level—and as we have seen—the scientific literature does not reflect and project the importance of the HUB as well as it should. So, even after we account for the ideological "training" served to a large portion of the Epidemiology community, there is still the matter that the information is not well publicized hidden.
Adding to the problem, plenty of people just…make shit up in their heads to rationalize their biases—or to avoid the cognitive dissonance sewed by the tailored brainwashing to which they've been subjected (schooling, media, institutionalization, etc.). In fact…get this, there are still people who think that taking an antiviral soon after infection is less effective at preventing respiratory symptoms than putting on a mask.


As we know from Asch conformity experiments, the inability to recognize the brainwashing comes from a variety of effects at once:
The desire to avoid social punishment,
The desire to climb the social ladder, and
Distortion of perception (not rare, but not extremely common).
We need not point to anything as dramatic as mass psychosis to explain these problems.
But the illusion of effectiveness is also spurred by a series of vaccine mandates that engineer differences between the vaccinated and unvaccinated cohorts. Between the military vaccination program and vaccine mandates targeting students and corporate employees, a skew of vaccine uptake toward healthy users was assured. Since the VSD likely excludes most or all members of the active duty military, it may underestimate the HUB among young Americans. Add on top of that, potential forms of reporting bias—this is not a theoretical point:

Given the circumstances, we must consider the likely possibility that the HUB was missed because it was part of an engineered process.
Engineering the HUB
The HUB gets missed because it is most likely an engineering effort by a well-connected and influential network, along with their ideologically driven underlings. There are honest people in the system, but they are largely ignorant of the inner workings of the system, or honestly terrified to speak out. Historically, there are also a number of suspicious deaths in the ecosystem, but that's a story for another day. This leaves few people left who can or will call out to the public audience about the trick that the Magicians are playing on them.
Remember the letter written by Fenton, Neil, Craig, and McLachlan to the ONS about bias and problems of categorization and classification (such as vaccine status) in the ONS data? Ultimately, the UK Statistics regulators agreed with the complaints from the quartet of data experts. This means that perhaps thousands of journalistic articles (including the sort that can be cited in Wikipedia) pushed flawed/invalid conclusions based on that data. Perhaps more concerning, millions (billions?) of social media posts based on those articles were a highly participatory groupthink exercise that ossified disinformation in the minds of both professionals and the public. It took only a few people to build the scaffolding of that grand illusion. The rest of the Big Picture was filled in by the imaginations of the audience.
In order to examine evidence of this effectiveness engineer process, consider all of the contributing factors to the HUB:
Conscientiousness correlates both with better health habits, greater education, greater wealth, and tendency to get vaccinated all at the same time. This is why the HUB = WUB = EUB.
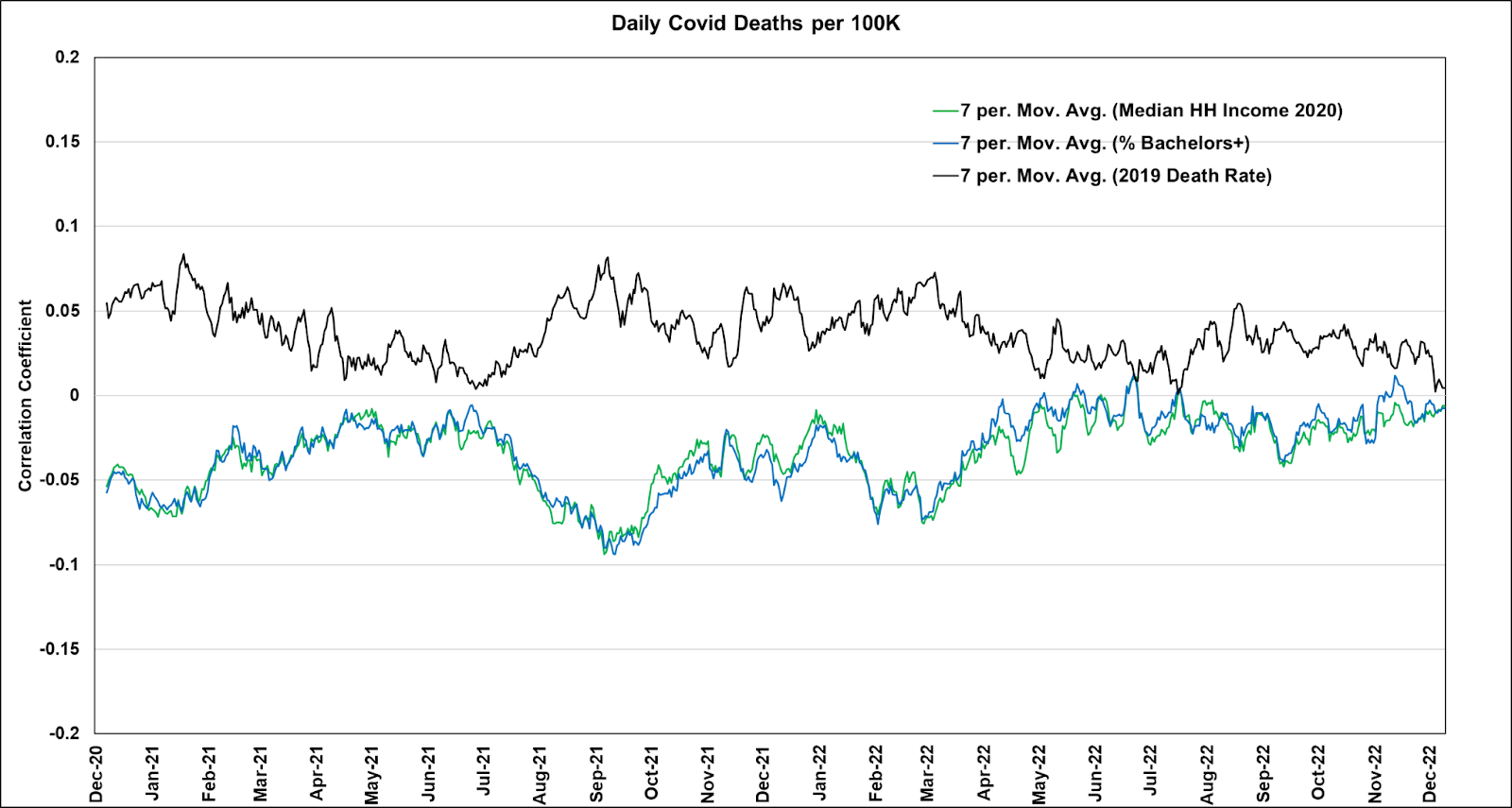
Poverty correlates oppositely as conscientiousness, providing a similarly magnetic relationship. Together, these effects polarize the data.
Mandates further polarize the data. The mandates targeted people most connected to "the system" which selects for or demands conscientiousness. This includes college students, members of the U.S. military, and corporate workers.
Fake vaccine cards add to the skew. Only the most healthy people are simultaneously aware enough, smart enough, or wealthy enough to credibly fake their vaccination status, taking healthy people out of the unvaccinated pool, and putting them into the vaccinated pool. I have personally heard of substantial pools of athletes who obtained or were encouraged to obtain fake vaccine cards.
For the purpose of a lot of government statistics, misclassification of vaccine status (not changing the status for two to three weeks after a shot) gives the impression of retrospective effectiveness. But these results contradict the group level data at the county. To reconcile the friction, we would need to believe that for every case stopped by a vaccine within a county, one was shifted to somebody who was unvaccinated, who would not have otherwise gotten sick. That is absurdity.
Those who want medical studies to look as much like RCTs as possible (which is misguided for reasons I document here and here) contradict themselves when they point to retrospective analyses that are strongly polarized toward extreme HUB effects. Once we recognize the HUB, and take it into account, the trials and the retrospective data look nothing at all alike. But many of the honest people in the system are either untrained enough to exercise it, under the mind control of ideological forces, or are too afraid to speak up.
Our current Surgeon General is another diversity hire. It’s apparent any time he opens his mouth. 🤦♀️
I have a biostats master's degree, which was extremely rigorous and difficult, basically doing calculus 8 hours a day for the first year, but I would argue that lack of math isn't truly the core problem. Academics often miss very simple things. In the first large project I worked on (as a graduate student), which was data from a computer-guided telephone survey of new breastfeeding mothers, the computer program contained an erroneous "skip" that caused the majority of women to skip past many of the vital questions to the end of the survey. Another student had worked on these data for 9 months (!!) and never noticed the immense amount of missing data.
Another project I worked on, there was a massive outlier in the data which completely changed the regression results depending on whether it was included or excluded. No one had simply plotted the data. It was a swarm of data points showing no trend but with one huge outlier driving the entirety of the slope estimate. There are statistics to identify outliers / high-leverage data points, but really, you just needed the simplest plot to see there was an issue.
Another project I worked on regarding mercury levels in dentists failed to control for mercury spills in the office, which was available data, but had been ignored. A mercury spill within the previous 6 months was a significant predictor of mercury levels and altered several models and conclusions once accounted for. No one had apparently read the entire survey and thought "Hey.... might this be a confounding variable?" Except me.
Speaking of confounding, ask just about anyone in academia what negative confounding is. They won't know. It's when there are two opposite trends which tend to co-occur. For instance, for one of my clients studying women in Kenya and their usage of professional midwives, having more money was a positive for hiring professional help, but having more children was a negative (because they were old hands at it by then). Well, women with more children tended to have more money, so the positive (money) and the negative (old hands at it by now) canceled each other out. Neither seemed related to the decision to hire a midwife, but that was incorrect. Both had to be taken into account *simultaneously* to see the true effects. Which is also true of healthy / wealthy / educated status and harms caused by vaccination; they are opposite effects on mortality, but they co-occur, so must be addressed simultaneously. It's negative confounding. Few in academia seems to grok this concept.
The stupid runs deep. But math isn't usually the problem in my opinion -- PhD statisticians adore mathematical models and want to outdo each other with the latest, most complex clustered-data time series multi-level sampling blah blah blah. Meanwhile nobody does effing scatter plots.
It's an inability to think with genuine curiosity, in my opinion, more often than it is a lack of rigorous math. I'm convinced academia now is deliberately churning out useful idiots because a system this complex and this corrupt needs a great, great many of them in order to run.