


Arguments Against Vaccine-Induced Mortality: Wrong Answers Only
The Chloroquine Wars Part LX

Since my articles (here and here) on vaccine-induced mortality made the rounds, and a bounty was placed on my head, some interesting things have occurred and not occurred. What has occurred is that I was put in touch with a number of academics, including some at top-five ranked research universities, making similar observations. In some cases, they are working toward publication, which is great, though the experimental vaccines face potential approval at the end of this month while our regulatory agencies seem content to pretend there are no safety signals and dodge all questions about why they're suppressing autopsies.
In some cases, research indicating vaccine-induced mortality and low-to-negative risk-benefit has been suppressed (here and here). Some very famous researchers feel under threat of physical harm for themselves and their families, with mentions of specific threats made. Such threats were made against Professor Didier Raoult last year, though U.S. researchers may have reason to take such threats even more seriously.
What hasn't happened is any serious kind of challenge to the data arguments themselves. We will take a look at those arguments that have been made, but first let's take a moment frame what our regulatory agencies should be doing to understand the problem.
Causality of Mortality
We have suffered through 18 months of Pandemonium during which all manner of absurdities have been thrust upon us. Two of those that stand out include, (1) the use of PCR testing at such high cycles that exponentially scale up tiny mistakes in sequence-matching to detect other genetic sequences, and (2) almost no autopsies have been performed.
Thinking about (2) is actually quite chilling. It makes no sense, whatsoever. Finding out from a friend that we've had robots standing by that could have been performing autopsies with blood analysis with essentially zero risk (far less than tending to an ICU patient or intubing somebody) this whole time, but that authorities apparently send strict "stand down" orders for those use of those tools makes me sick to my stomach. Meanwhile, vaccine-induced death causality has been done in Europe, pointing to large numbers (here and here), though that information has been suppressed and denied in the U.S.
Of course, this overly strict requirement of "proof of causality" (by regulatory organizations that seem to be sabotaging the process in service of an industry that works in tandem with media that sabotages clean information signals) comes during a pandemic in which a positive PCR turns falling off a ladder into a COVID death.
Unrelated reminder that multidrug early treatment regimens save nearly all COVID patients.
Many of those not paying attention or not capable of paying attention build cognitive dissonance throughout the process. Perhaps that explains the following flimsy arguments.
Arguments Against Vaccine-Induced Mortality: Wrong Answers Only
I'll start with Economist Steven Postrel.

I've debated with Steven a few times (or observed him debate against my points while I was unable to discuss due to Facebook bans) before and feel he makes quick judgments before deeply examining many complex topics. Of course, we all do that to a degree [because it's economical to have fast/slow thinking gears], but in conversations during the pandemic, he seems to jump to justification by authority on such topics instead of expressing interest in seeing the work, then not respond to deeper discussion [when I've done the actual work].
I'm not a fan of using terms like "alarmism" in association with data, and I don't think I've used alarmist language relative to the observations, but it is noteworthy that he does not at all argue the data. I sent him a PM asking what the "official number of vaccinated COVID-19 deaths" is, but he did not respond. I will note now that everyone I've asked, in government and academia has either not answered the question or given a different answer. Every single one. That includes most recently a conversation with a Ro Khanna staffer who told me that there were zero deaths caused by vaccines and incorrectly claimed without citation (in fact, all she made were uncited statements during a half-hour call) that (official) numbers were similar around the world. This seems to be what happens in a world in which the CDC confidently makes statements that aren't actually about real numbers (the made up 99% number, for instance), and suppresses all attempts at attaining that data, and nobody in Congress or the press ever even asks questions.
It depresses me to see a libertarianish economist doing exactly nothing to push the government on the veracity of its data claims. I would also welcome a more serious argument by Steven.
Many who have taken shots at my analyses misunderstood some of the numbers. To be fair, I gave only enough explanation that experienced data minds would understand easily.


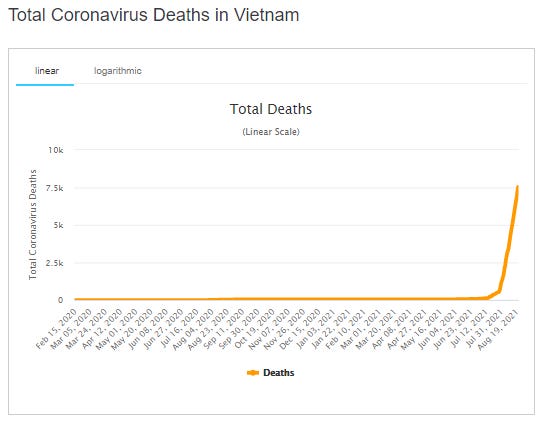
The "implied mortality" numbers in my "naive nations analysis" take currently unresolved cases and apply the post-vaccination-start CFR to estimate future deaths from those cases. I've used this estimation method many times during the pandemic and it has consistently worked out well in prediction models. In the case of Vietnam, my estimate proved slightly low this time, which raises the mortality per dose results.
Another wrong answer comes from Taison Tan:


Testing is a long and tricky conversation that would be worthy of its own deep dive data article. However, there is not likely much link between mass testing and symptomatic cases, and far less with cases that progress in severity or death. But most pertinent to the point is that the CFR analysis on Europe involves an 18-day case lag (the denominator) where COVID deaths (the numerator) drive the broad rise in CFR. The rise in CFR took less than three weeks during which there was no broad change in testing regimes.
I'd be open to seeing somebody take on my two analyses based on testing regimes most of all because I strongly believe they'd find no significant effect. It is a well-understood publication bias that suggests that papers are less likely to be published when they do not confirm researcher predictions or desires, so to the extent that we do not see such an analysis completed, we should update our priors in a way that supports my analyses.
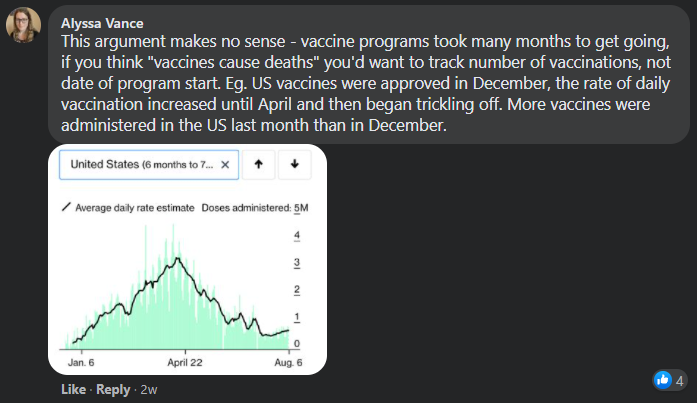
Google software engineer Alyssa Vance makes the argument that my identified vaccine mortality estimates don't match the vaccination program rollouts. Aside from the fact that she posted U.S. vaccine rollout rates (which differ significantly from European nations) I don't think she read my argument well enough to really absorb it. Since most of the vaccine-induced deaths (like COVID) come from the elderly (on a fairly extreme distribution), we need to take a look at vaccine rollout as a vector, not a single scalar. I confirmed in the OWID data set that I used that vaccine rollout among the most elderly groups matched the CFR rise I noted. My claim is easily falsifiable, but nobody is arguing that. Here is the UK rollout curve as an example:

Again, I welcome outside analysis of the data, but please do the actual analysis. I strongly believe outside checks will reconfirm my results. In fact, my spreadsheet has been passed around among data geeks and university researchers with no complaints to this point.
Matterport Founder Matt Bell joined that save conversation on Facebook, which I could not participate in due to being censored there.
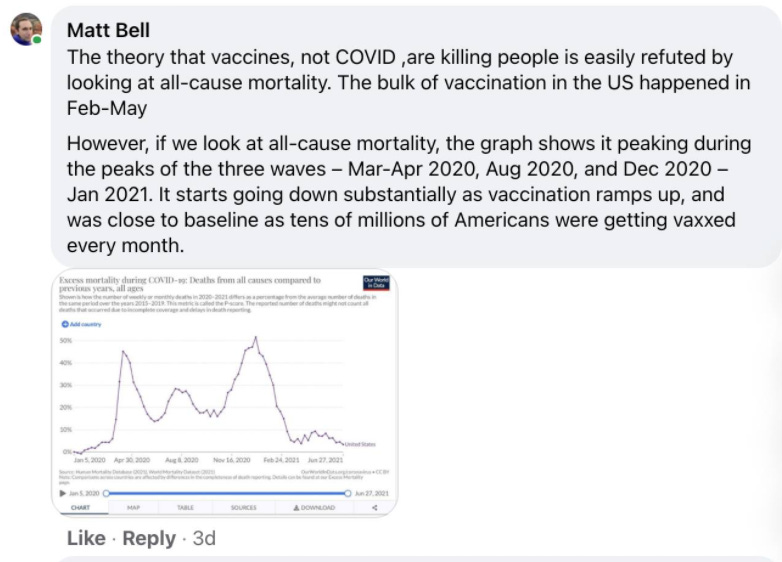
Matt's argument is interesting in that, as stated, it should apply to all deaths. All deaths are easily refuted because "this chart would look different if they existed". It's a bizarre argument, but I can see how he manages the self-deception. It starts with assuming that I'm wrong. What his cognitive dissonance doesn't allow him to see is that the vaccine-induced deaths are already part of this chart. They were simply categorized as COVID-19 deaths, which I explained in my analysis, which I'm guessing he didn't actually read.
Here he makes the same fail that Alyssa did, not focusing on the vaccination of the elderly, which absolutely fits my analysis. I invite him to download the OWID data, compute an age-impact vector from the VAERS numbers, and perhaps actually perform the analysis before assuming the result.
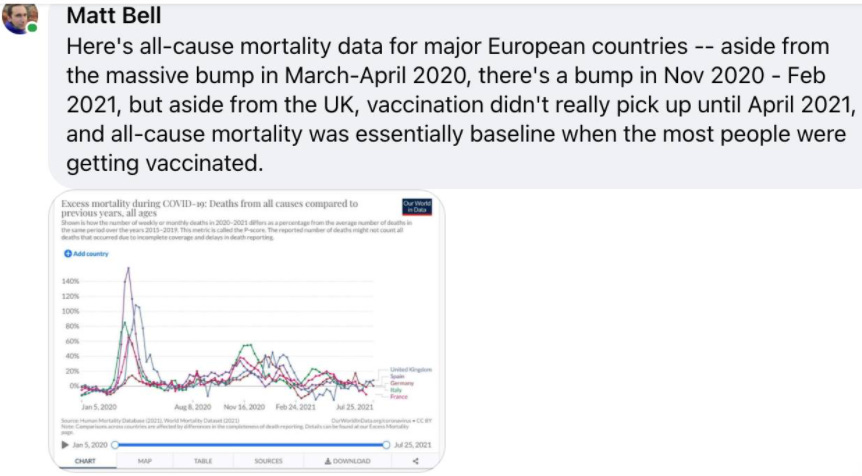
Addendum: While most of the focus of my European analysis is on the elderly, because that's where we see the signal of larger numbers, it is also worth noting that many signals have pointed toward increased excess mortality among the young (here and here for instance) once vaccination campaigns reached them.


Additional Observations
I answered a few other weaker arguments here, though they likely aren't interesting enough for most people to want to wade through. A couple were deleted by authors with credentials to protect because (I assume) they were made to look foolish. Wish I'd saved them.
A few dozen statisticians and data scientists read this newsletter/blog, but none have offered observations of flaws, though one very good scientist I've worked with some this year is nearing publication with a substantial-but-lower mortality estimate based on U.S. data, and I will mention that my own currently-incomplete analysis of U.S. data points so far to a substantial-but-lower mortality estimate.
It is time that the U.S. regulatory agencies (CDC and FDA) come to the table for real discussion, or that we write them off as corrupt, extralegal organizations. What other choice do we have?
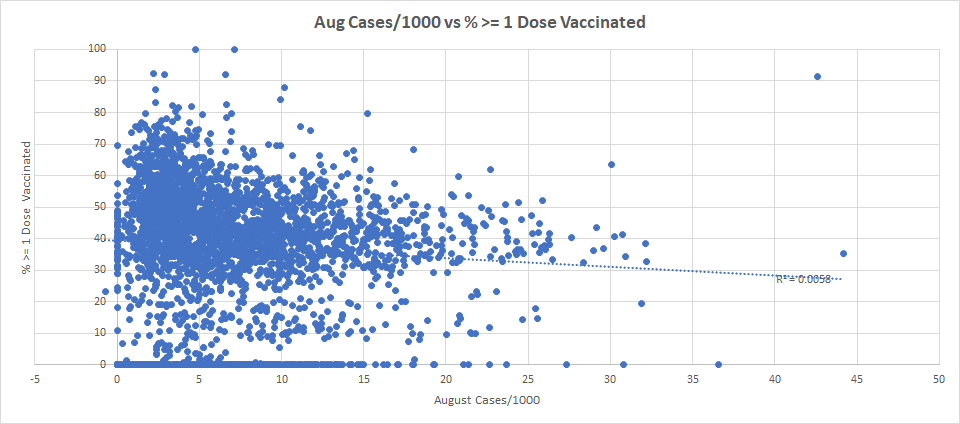
Meanwhile, your moment of Zen: There is no [significant] correlation between rates of COVID cases in U.S. counties and vaccination rates (Texas numbers excluded here, but on their own show a similar result). I am thinking through theories that might explain this result and will write more about this in depth in a future article.
Hi Mathew,
I am repeatedly hearing the media blare, "the vaccine is ~99% effective against hospitalization etc." Yet I also see the rapidly declining indications of efficacy in UK and Israel, where ~40-60% of hospitalizations are among the vaccinated. I find it implausible that there would be such stark differences in case rates, even accounting for differing levels of vaccination. I'd love your take on this. ie, do you trust this data? (and I don't mean the Cleveland Clinic data referred to which used an irrelevant timeframe to make such inferences, that is clearly bullshit, I mean the more recent claims which are too numerous to even bother citing).
The only thing that I think could skew it that much, aside from outright fabrication, is that the tests in the US are run at different cycle thresholds among the vaccinated vs the unvaccinated. But that, too, seems like it would be difficult to pull off logisitically. ie, a hospital gets 100 sick unvaccinated people, and orders PCR tests at 40(Ct) and finds 99 of them are positive, vs 100 vaccinated people and orders PCR tests at 28 (Ct) and finds 1 of them is positive. While that is what would happen if they did such a glaringly manipulative protocol, it would take implausible (to me) levels of coordination to make sure all these hospitals treated the testing so asymmetrically. Am I wrong about that? What is your thinking on the issue?
It requires mental force for me to stay open to the fact that these data could be legitimate. My bias to distrust the official narrative is nearing calcification, which has its own dangers, and I want to be weary of that. But either way, even if it as remarkably effective at preventing severe cases as 99%!, then shouldn't the vaccinated feel highly assured in their safety and not exposed to undue risk by the unvaccinated? ie- WTF would the rationale be for mandates/passports etc if the vaccinated were afforded so much protection?
Something doesn't add up and I need help figuring it out. If I had to boil it down to one question, do you trust these claims?
I am not surprised at all by the superficial critiques leveled at your analysis. The barrier to entry for these conversations is high and if you don't have a robust statistical background (or the desire to learn), then most people have to take the approach of "the media tells me this is laughably false, so there has to be an obvious mistake in the methodology." Unfortunately, after years of research into various unrelated topics like cosmology, history, etc, I have come to realize that almost nothing that gets promoted as "conclusive" in the mainstream actually has the necessary legwork backing it. Most folks are content (whether through lack of time, cognitive dissonance, or fear) to believe that "people smarter than figured this out." Which is partially amazing because I also think most people of average or greater intelligence are also aware of the conflict of interests in our corporate media, medicine, government, etc.
I believe the extreme specialization of knowledge plays a large role in this... most people, by necessity, are very familiar with their own little niche and have very little exposure to information outside of their particular sphere (this obviously contributes to the Gell-Man effect, described a few articles back). When one considers this specificity within the medical industry alone, for example, just within the last half century or so, the average person has gone from having a primary physician who handled essentially all of their maladies to the point where their main doctor more or less just exists to write referrals to other experts, so every person has a full team of medical authorities responsible for their health (to say nothing of the issues that arise when we outsource responsibility for our personal well-being to third parties who have, no matter how well-intentioned, a profit motive).
So, most of us don't have the time required to fully understand a wide range of topics, so many attempt to assess validity by judging the analyst's character nstead of reviewing the data (and the quality of said data). This I further compounded by herd mentality and not wanting to appear as a foolish tin-foil hat nutter. The funny thing is, I have some very unorthodox opinions and I also do not subscribe to grand, unified conspiracies. Certainly, concealed agendas and propaganda do exist, but for many topics, it's as simplistic and naive to believe in hidden cabals making world impacting decisions as it is to believe the mainstream narrative. Paradigms, which arise both organically and with motivated assistance, sort of take on a life of their own. Essentially, I think the problem is a symptom of over-organization and historically, this is what contributes to the fall of a civilization. We create a complex machine with very specific parts that are not interchangeable and the focus shifts to filling these precise roles, at the expense of general understanding. So, contrary to much conspiratorial thinking, the problem is that eventually there's no one pulling the strings because everyone's forgotten how to do so, lost in the minutia of specificity. Compound this with a culture that values brevity above accuracy (Twitter and it's character limit is a wonderful sign of the times) and I believe that analytical "mistakes" on the level of what is described on this substack are to be expected as the rule, not the exception.
Apologies for my rambling, as I review more of the data and analysis here, I hope to be able to contribute in a more direct way. There are certainly enough red flags in the data I've reviewed over the last 18 months to cause me to reject most of the "accepted" premises of this pandemic, but I haven't applied the sort of statistical analysis done here in a couple decades, so I have a lot of mental cobwebs that need clearing. But even just a cursory review of the VAERS database should alarm anyone with even a basic knowledge of math, it's hard to hand-wave away AEs and deaths that are at least an order of magnitude higher than all other vaccines combined (which appear to have about the same total amount administered when compared to the total COVID doses). And I don't believe that assuming that the COVID vaccines AEs are recorded more consistently than AEs from other vaccines would be enough to get them to a similar level of safety, especially in light of reports that COVID vaccine AEs have been encouraged to not be recorded. Like Matthew though (and I think most who are interested in researching this, contrary to "popular opinion"), I do not want this to be the case... I'd rather not live in a world where a dangerous, un-approved, ineffective experimental gene therapy is promoted and mandated. In another classic case of projection, the "follow the 'science'" folks somehow think that the people who point out potential hazards are suffering from a form of wishful thinking... which I can't help but find incredibly odd. At no point in my life did I want to be a contrarian who disagrees with virtually everything presented by traditional academia via the mainstream (and social) media. It's frankly exhausting and certainly a lot harder than simply wearing a mask and getting a couple shots. If I was going to pick something to have "wishful thinking" about, I'd pick something a lot better!