
What Risk-Benefit Analysis?!
The Chloroquine Wars Part XLIII

One of the disturbing aspects of the mass vaccination program happening under an emergency use authorization (EUA) is the lack of risk report and lack of risk-benefit analysis. These would ordinarily be legally required for such a program, if I understand correctly (please correct me if I am mistaken). Informed consent cannot truly take place without a risk-benefit assessment.

While I would like to put together my own risk-benefit analysis, the task is a tall order given how little authorities and vaccine sellers seem to care about reporting on the risks. So long as they are not required to open such a report up to critique and debate, they have no incentive to do so. And everyone involved in allowing that to happen is responsible for a terrible decision (sorry Trump fans...and Biden fans).
Previously I used the PHE data to demonstrate the shockingly low mortality benefit to very young vaccine recipients. So, I decided to go a step further and run the numbers for overall mortality benefits under what seems like a reasonable set of assumptions. As with my PHE data analysis, I would be foolish to think that I know the values of all of the parameters, so I will present a range of results based on a few parameters.
The Setup (read only if you care about the modeling):
I chose to make a few simple assumptions. I can go back and make these variables, but they will have little to no effect on the overall results (but might change subgroup results). Let's call this an instinctive Pareto distribution. I've handled the numbers enough to know this isn't terribly far from accurate, and this exercise does not actually require exceptional accuracy.
I categorized 80% of the population as "low risk".
I categorized 15% of the population as "median risk".
I categorized 5% of the population as "high risk".
I threw 5% of deaths into the low risk group.
I threw 15% of deaths into the medium risk group.
I threw 80% of deaths into the high risk group.
For the last three, this is for both COVID-19 and also proportions of vaccine-induced deaths. My look at VAERS data 10ish weeks ago suggested a highly similar age-risk curve, so until I see a better fleshed out curve (We're waiting on you FDA/CDC/Manufacturers), I take this as a reasonable comparison. I doubt it makes much difference in the big picture I present here.
I chose for the moment to ignore one-dose vs. two-dose distinctions for simplicity. Perhaps I'll go back and add that in, but the results seemed not to need that kind of breakdown. I used 50% as the rough approximation of mortality efficacy I imputed from the PHE data using the most reasonable guesses at my parameters there. I may go back and turn this into a variable. It will make a difference, but again, the larger case is made without it.
The Variables
For the purpose of this exercise, I left variable each of the following:
[True] Vaccine deaths per million fully vaccinated
Percentage of vaccine deaths specifically due to Type II COVID-19
Case fatality rate (CFR) of cases moving forward (I think this is where the CDC goes wrong)
Proportion of population moving forward who will suffer from COVID-19 [during the time period when vaccine immunity is expected to last]
The second of these assumptions does not affect the risk-benefit analysis, but I wanted to see how if affects a re-computation of vaccine mortality efficacy after including Type II COVID-19 deaths against the vaccine efficacy measurement.
Some Basic Results
When I see vaccine advocates claim vast net benefits to the vaccine program in online discussions, this is what I suspect they imagine: the vaccines cause perhaps 10 deaths per million, but save perhaps 1,000 lives per million vaccinated under the assumption that 10% of the population would suffer from COVID-19 without vaccination at a 2% CFR:
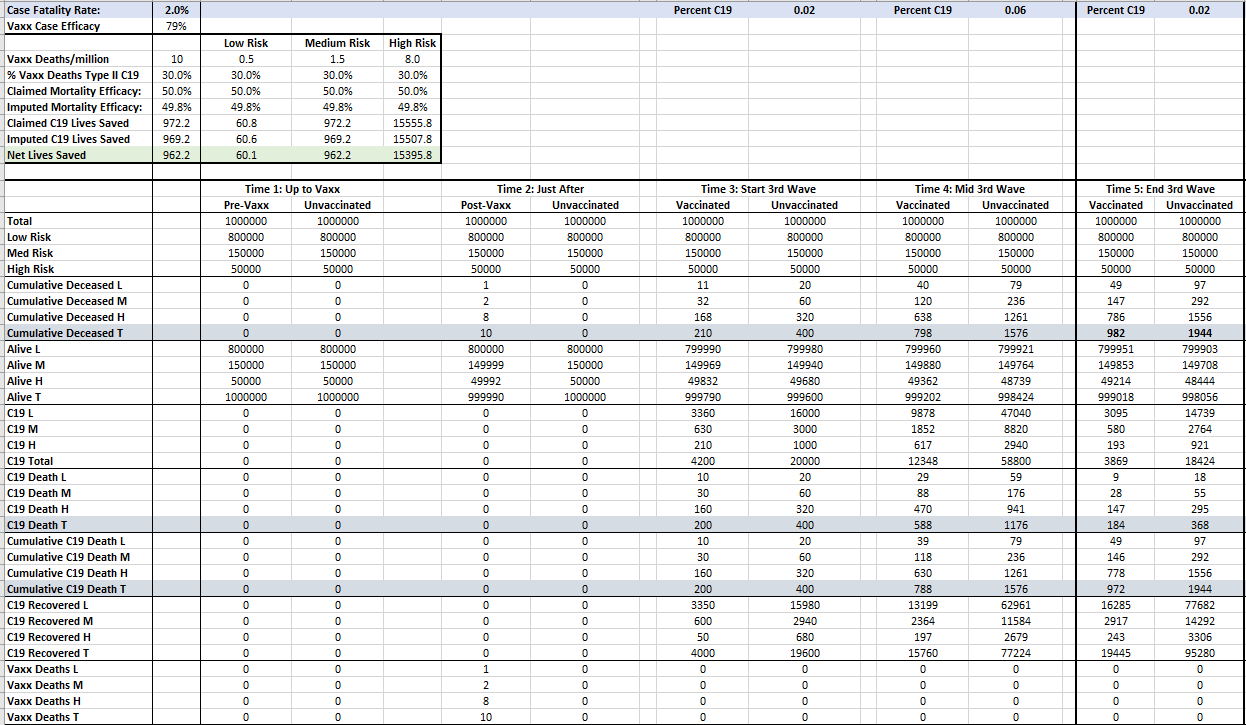
Okay, let's zoom in to the important part. All numbers are percentages or totals per million people fully vaccinated.
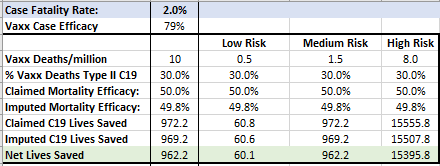
If the the next waves results in 10% of a population getting COVID-19 with a 2% CFR, the vaccination program looks worthwhile on the whole, though we might want to them zoom in on the low risk group to stratify those results because I still suspect the children look like human shields for the high risk group (ahem).
Now, let's change the numbers up. From the PHE data, I computed a 92.7% reduction in CFR for the Delta variant that now causes 99% of COVID-19 cases in the UK. Let's run the numbers under the assumption of a Delta wave with CFR 0.15%.
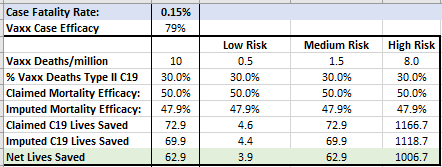
It still looks like the high risk group clearly gains a net-benefit from vaccination (can somebody explain to me why a ring vaccination program was never discussed?), though many or most among the low risk group gain little to any benefit. A discussion of net-benefit for the medium group would involve wading into a variety of topics that get increasingly complex including long haulers, a full list of AEs, and even ADES and leaky vaccines.
This scenario however involves 33 million more Americans getting COVID-19 during the period of efficacy for the vaccines, which is roughly the number who have already had COVID-19. But many Americans now have immunity and perhaps the most vulnerable and those at the centers of social networks are the most likely to have had COVID-19 and recovered. Also, that's from both of the first two waves. What if we reduce the coming wave to a fifth that number of cases. This pattern fits some observed viral wave propagations such as the Spanish flu in particular. The results:
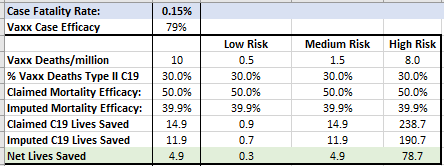
Now let's examine the case where Steve Kirsch's estimate of 25,000 lives taken by the vaccines is correct. That relates to perhaps 200 lives per million based approximately on when those numbers were compiled.
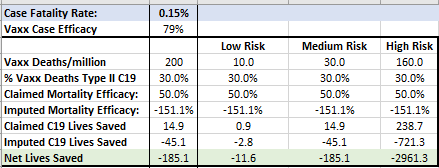
This clearly doesn't look good for anybody! Not only that, but the implied mortality efficacy for the vaccines is now negative (based on attributing 30% of those deaths to Type II COVID-19).
Maybe you think 25,000 deaths is too high. Let's try a fifth of that…
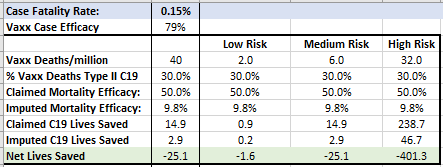
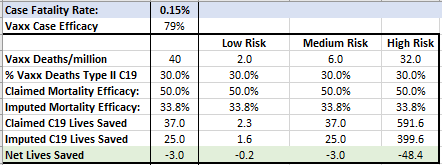
I have to admit my surprise that the case against vaccinating those in the high risk group looks the worst under what seems to me like a reasonable set of assumptions. I'm going to go ahead and bump the COVID-19 cases up to 5% from 2% just to see how much a larger-than-expected wave affects the final numbers. It still doesn't look good.
Here are some things that are clear to me throughout this exercise:
The net benefit to the low risk group, which represents 80% of Americans, only looks (modestly) good under the assumption that the vaccine program begins at the outset of the entire pandemic, or that the remaining impacts look the same as the past results.
The case for vaccinating all the children looks even weaker given the 100 to 200 cases (sexes grouped) of myocarditis per million in part of that age range.
The net benefits clearly go quite negative if the coming wave is less deadly.
The net benefits go gruesomely negative under sets of circumstances that I cannot rule out and look quite reasonably close to what we're seeing.
Now, the question is, have the responsible authorities done this analysis and found the claim of net benefits dubious, or have they not even bothered? Neither answer is good.
Alex Berenson noted in the 6-month follow-up report by Pfizer on their trial there was no reduction in deaths on the vaccine compared to the placebo group:
https://alexberenson.substack.com/p/blocked-again-for-a-week-this-time
Robert Clark
"According to a new pre-print study, boys between the ages of 12 and 15, with no underlying medical conditions, were four to six times more likely to be diagnosed with vaccine-related myocarditis than they were to be hospitalized with COVID."
https://childrenshealthdefense.org/defender/adolescent-boys-risk-hospitalization-pfizer-vaccine/