


These Vaccines are Ineffective: A Play in Three Acts
The Chloroquine Wars Part C

"And I think it's because good cons are all based on the victim's need, and the successful con artist is the one, I guess, who can exploit that. I remember reading something about this, that one of the great traits of confidence tricksters is the level that they flatter their victim." -Alfred Molina
IT'S TIME TO DROP BOMBS!
I never conceived of writing a hundred articles in this series, and there are more series offshoots, but here we are. The world is spiraling further out of control, and the situation is only getting worse.
I am still managing fallout from a complete home flooding, and will be for several weeks, so it is hard to keep up with all of the topics I would like to analyze and document, but today I took the step of interviewing with Steve Kirsch to at least lay out the story of the false evidence of vaccine efficacy. In doing so, I introduced several pieces of the story that I believe will be new to many people, including even RTE readers.
Immunodeficiency and Autoimmune Disorders as the Hidden Comorbidity
I am working on a long form article (or multiple parts) to lay out this topic, but this requires reading and synthesizing dozens of studies. Even with the help of my wife, a biochemist, geneticist, and bioterrorism specialist, this takes substantial time. Just know that it's coming and it's important. And by important I mean it's the 37th reason you should strongly distrust authorities pushing the official narrative. I'll go ahead and spoil the result now and back it up later: almost everyone who dies from COVID-19 has a critical immunodeficiency or autoimmune disorder. These may include one or two you've never heard of, even if you are a healthcare professional. This throws all risk-benefit analyses of vaccines out the window for healthy individuals.
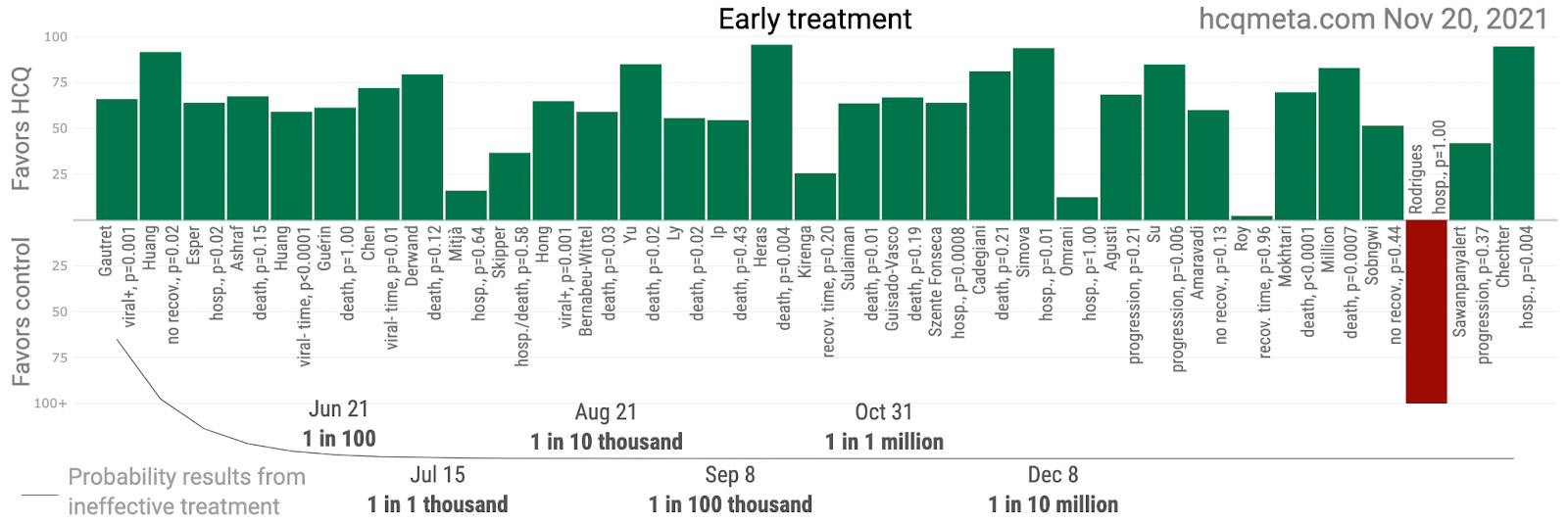
It may also derandomize the vaccine trials. While participants were sorted for a subset of conditions associated with immune dysfunction, they missed a lot of the most important conditions. Though to the degree it does derandomize the trials, I personally don't think it matters much, to be honest. With arms that size, the only thing that matters is that the deck wasn't stacked. In other words, I'm just as comfortable with OTCs and RTCs for most purposes---dependent upon trial design, of course. And since there was a negative all cause mortality benefit (H/T Alex Berenson for the update) in the Pfizer trial, the deck likely wasn't stacked. However, finding out that the Pfizer trials were not "well run RCTs" will give the RCT fundamentalists fits. They either have to now denigrate the vaccine trials, or accept the entirety of the vast mountain of hydroxychloroquine efficacy data (here, here, and here as well as several other places at RTE). Because...we all really believe they just sort of don't see that mountain.
"We wanted it to work!"

But somehow, wishes were granted when vaccines,
Suddenly cured coronaviruses for the first time,
Suddenly worked as mRNA gene therapy for the first time, and
Solved a pandemic for the first time? Oh, was there one? I don't think so, but post it in the comments if you like.
Major Issues with Pfizer Trials
The vaccine trials have all been conducted as black boxes---to the point that many of the decisions have been made without logical respect to the claims of the trials. For instance, the Chinese vaccines claimed 100% efficacy against severe COVID-19 and death. You probably never heard that in the media, huh?
But more importantly, and closer to home, the Moderna trial was a total black box, so we have to focus on Pfizer. Of course, these companies seem to have so much lobbying sway that our government may help them hide documentation about these trials for up to 55 years! As Aaron Siri, who is doing tremendous and important work, points out,


I strongly suspect that when the Pfizer data comes out (when I'm 99 years old?), we will find from the raw data that the entire efficacy claim is constructed from process, not medicine.
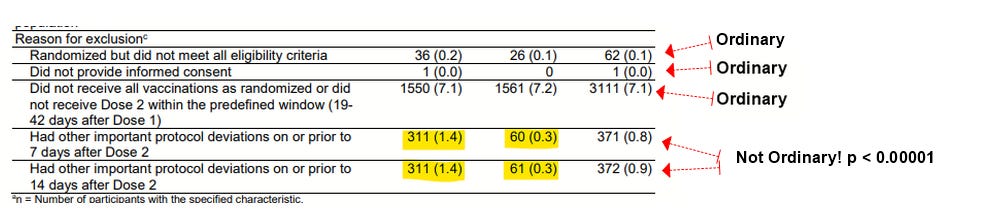
While I mentioned that the Pfizer trials were not really RCTs, the larger point is that they were not double-blind as those who parroted "well run clinical trials" seemed to suggest. Ventevia whistleblower Brook Jackson was fired for reporting such Pfizer trial problems to the FDA as outlined in the BMJ (Thacker, 2021). Among these problems included casual unblinding of the trial, though you should really listen to David Wiseman explain the story on a more detailed level. He is detail-oriented if anything, and one of the unsung heroes of the pandemic, on the scientific front lines of half a dozen major stories.
I'm going to stop typing now and go back to compiling research, so here is the interview with Steve:

Note that I'm not the only person who has come to the "basically zero efficacy" conclusion. Professor Norman Fenton has reached this point from a different angle.
But...But...Waning Efficacy is the Problem---We Just Need Boosters!
There was never waning efficacy. Even Jeffrey Morris can tell you that.
Okay, sure, maybe the Israeli data was fixed? Were I to fix data, I would do so along risk-stratified subgroups, so that's certainly possible!
So, if the data was real, it contradicts the story that booster shots were needed. Either way you want to call it, there's no need to take this vaccination program any further!
What did wane was the effect of survivor bias and selection bias (including informative censoring in the retrospective trials). Either that, or the vaccines introduce new levels of immunity dysfunction. Either way, the situation is not good.
This won’t be over until it is societally acknowledged through life insurance applications having a box for Covid-19 Vaccination and a “yes” check results in higher premiums for the applicants.
Assuming, assuming, the data are legitimate, vitamin D3, or sunshine, fresh air and warm climate must somehow control the outbreak of rowuhan. Why do I say that?
Look at the vax rates in Queensland, Western Australian. Canberra, South Australia, Victoria, NSW, Tasmania, and NZ. Although their rates have not yet reached the levels of NSW and Victoria, there is no logical explanation for days of zip cases in WA, SA. and Qld. Canberra had cases in the teens yet it was the first place to reach double vax rate of 90%. In contrast, cold and wet Europe have massive increases despite having lower vax rates than in Australia.
Seasonality and regionality, combined with the weakened immune caused by the vaxes and the vaxes themselvesa re the causes of the European outbreaks. Without the introduction of the vaccines, their cases would be lower and milder due to acquired immunity from 2020!
A reminder that "cases" mean nothing if people don't need medical care and die.