
Hiding the Truth by Hiding the Data
The Vaccine Wars Part XLVI

A few days ago I read one of Jessica Rose's most recent articles discussing Pfizer vaccine trial "safety" documents. One thing that jumped out at me with respect to this study protocol document (with an unwieldy name and an even more Byzantine protocol set) was how the method for reporting adverse events (AEs) conflicts with the nature of some AEs (particularly SAEs), and death in particular:
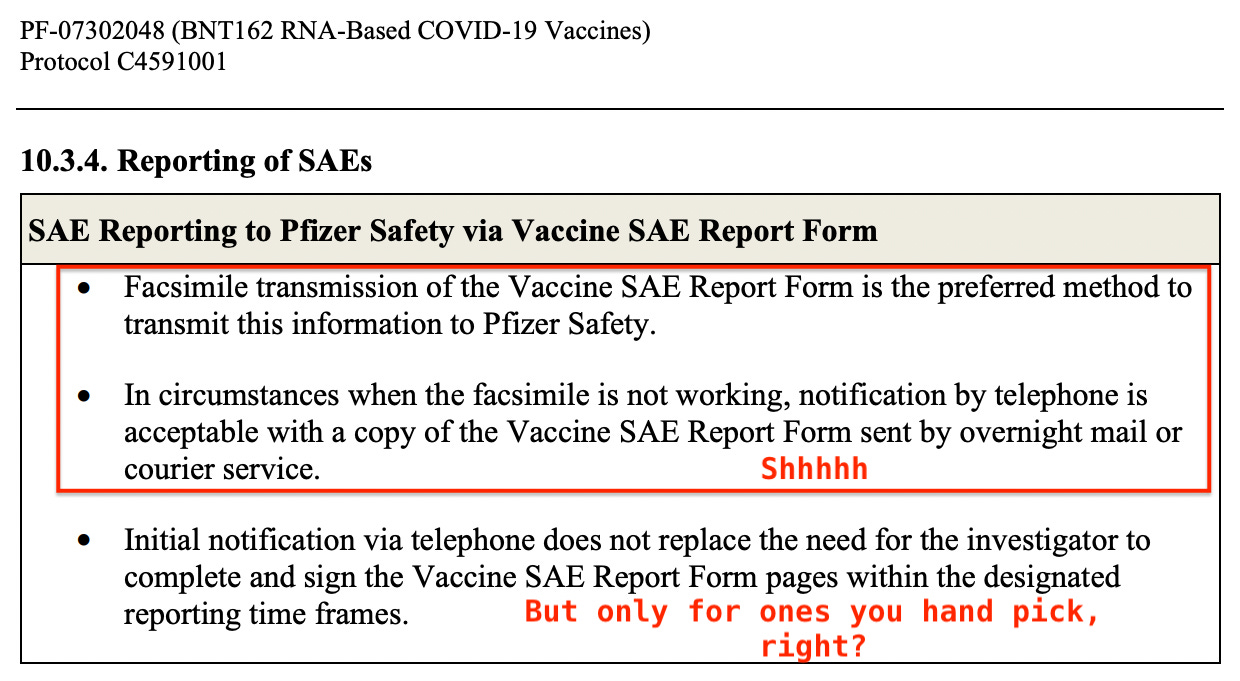
They wanted fax reports? And secondarily phone or overnight mail?
If I didn't know better, I would think this stands out as experiment design for the purpose of suppressing data. All three methods, none of which involve something like a simple email, stand out as both (1) unnecessarily time consuming and (2) lacking in a good record trail.
I will assume that some RTE readers are highly conscientious people who always perform all their paperwork perfectly, but most of us weigh time spent on bureaucracy against our economic interests. Time is valuable. I mention that not to debate values, but to make it clear that we should expect a substantial portion of AEs to go unreported under this system.
In fact, I would think SAEs, and death in particular, would more often go unaddressed by this system than simpler AEs, but under difficult circumstances, time is even more valuable.
Let's remember that the vaccine partisans have been telling us that we cannot draw conclusions from the VAERS database because the proportion of reporting is unknown. By that same logic, Pfizer has crafted an experimental protocol that defines away safety signals.
Is there any way at all for the trial managers to know whether or not they have all the important data from which to draw conclusions? I can't see an easy answer, but the strangely archaic form of communication chosen suggests the prioritization of crossing the finish line with a well type setted trial report document more than a data summary that matches reality with any fidelity.
These are Not Trustworthy Authorities
If there is any primary lesson during the pandemic, it's that unchecked proxy trust opens us up to critical failure. We are living through the unannounced era of Healthcare 2.0. The internet changed the game for every industry, but in different ways. No other industry dedicates more of its budget to advertising and propaganda than the Pharmaceutical industry, and no other industry is better joined with the government systems that might regulate it, save the obvious example of the military industrial complex.
Let us summarize the instances of data engineering, withholding, falsification, and sleight-of-hand that we know about. I'm sure I'm missing some:
Excluded Data. The lopsided exclusions that I noticed almost the moment the Pfizer trial report went public, and reported about in April 2021 shortly after starting this substack, have still never been explained. A few months after I showed that to Steve Kirsch who later found the same thing in the Pfizer vaccine trial on children.

Excluded Cases. Cases from the Pfizer trial data such as this man who died shortly after being vaccinated, but was excluded from trial results are popping up. It's chilling to think about it this way with respect to the data exclusions: 1 down, 249 to go.
Manipulated Cases. Other cases of patients seemingly jerked around and vindictively targeted at some trial sites.
Trial Fraud Lawsuit. The Brook Jackson trial fraud case. This case calls into question the whole of vaccine trial data, and raises more than a few questions about the entire biomedical research industry.
Poor Trial Blinding. If it wasn't bad enough that the trial blinding was terribly insecure (here and here), total unblinding reduced the time horizon to the point of making the data almost meaningless, not to mention unethical (Stoehr et al, 2021). This saddles us with debates about the need for boosters to cope with waning efficacy, which circularly relies on the tenuous assumptions of safety and efficacy (but might simply be explained by reporting delays or data miscategorization).
Questionable Trial Activity. There are reasonable questions about the exceptional recruiting results at a trial site in Argentina.
Extending Trials to Avoid Failure. In order to dodge a negative result, Pfizer reopened recruiting and performed their trial on children during a second time period. The results should not be aggregated for multiple reasons (protection against one strain may not imply protection against another now that we've shifted to the Omicron era), show sparse benefit, and that sparse benefit may be the result of a lack of risk-adjusting of person-days.
Questionable Assumptions and Calculations. Some of the research supporting child vaccination is based on seemingly impossible claims.
Defining Away Safety Signals. Though the CDC wrote up a flimsy and flawed protocol for evaluating vaccine safety signals, they eventually admitted (claimed?) to never using it. Perhaps that's why they were months behind others in detecting elevated incidence of myocarditis and other heart/cardio problems. I have to ask "claimed?" because there is probably no way to even find out if they were ever running the numbers, but trashed the reports.
Proxy Metrics. The uncritical assumption that antibody titers [away from the epithelial surface of viral entry] are a highly meaningful metric of efficacy.
Hiding Data. The CDC admitted in February to withholding other critical data related to vaccine safety and efficacy.
Hiding Data. The CDC has withdrawn the publication of statistics it was previously reporting publicly.
Cherry-Picking. While waiting to give my VRBPAC talk in April, I noticed that data sources for the graphs presented by Dr. Heather Scobie included only a fraction of 1% of U.S. jurisdictions. Given how much data the CDC should have, this strikes me as likely similar to the statistical sieves in both the Vaccine Safety Datalink report and the ONS data.
Questionable ONS Data. Professor Norman Fenton demonstrates that the impossible results can only be explained by extreme selection bias or a very dirty data set on top of systematic undercounting of mortality during the early vaccine rollout.
Revised Data. The CDC substantially revised its statistics on the number of people actually vaccinated, but without ever noting the dramatic implications associated with computations of efficacy.
Inconvenient Insurance Analysis. Startling insurance data in the U.S. and also in Germany goes ignored, and gets buried.
Inconsistent Results. The lack of consistency in state level vaccination data COVID data calls into question CDC presentations that consistently show oddly pristine results.
Autopsies? The general lack of autopsies during the pandemic and vaccine rollout stand out as suspicious. While trillions of dollars were spent during the pandemic, autopsies were not part of the funding. When a German pathologist examined bodies and found a substantial number to have died due to vaccination, enough pressure was put on him that he crawled into a shell. Other pathologists have found similar results. Note that robotic autopsies (a.k.a. "virtopsies") are more accurate and less corruptible. There are some limitations, and a few reasons why a live pathologist might recognize COVID-19 or vaccine damage better, but the availability of virtopsies would provide a significant new data source. Also, nobody would have to fear infection (which was more a fear early on during the pandemic).
The DMED Saga. The FDA, CDC, and DoD seem to be aligned in ignoring the obvious changes in military health databases despite the DoD being a partner in the CDC's Vaccine Safety Technical (VaST) workgroup.
No Credible Risk-Benefit Analysis. These many problems add up to reason to leave extremely wide bands in any published risk-benefit analysis, and state that any such analysis is incomplete and ongoing.
Differences by Kind. The selective use of antigenic testing.
Ignoring Data. All Cause Mortality in Europe is skyrocketing among children. Public Health authorities and regulators remain silent.
Modeling Assumptions into Conclusions. The use of models to assert the appearance of efficacy rather than real data has driven illusions of efficacy. Most people see a nice picture and do not know how or why to follow the source and read the description of such graphs.
Double Standards of Classification. While the COVID-19 pandemic was ramping up, anyone who tested positive just before or after death was deemed a COVID-19 death, but strict "proof" (which is not even a concept in science) was required to demonstrate vaccine-induced mortality, with no standard or attempt at gathering evidence to meet a standard.
Coding Logic Errors. The CDC removed 72,000 COVID-19 deaths, including 416 deaths of children due to a "coding logic error", which conveniently gave a window for Bloomberg to publish an article claiming that COVID-19 is deadlier for children than influenza, which is false.




Note: This list has been and may continue to be updated from the original.
This list might be longer, but judging from the Pfizer data document dumps, nobody at the FDA bothered to work with the material enough to organize it in even a basic way. And, of course, we still don't know either the full contents of the vaccines, much less the placebo used during the vaccine trials, which somehow managed to result in 8 hospitalizations among kids.
As attorney Robert Barnes appropriately notes: "If they're lying about this drug…how can they trust the FDA on any other drug?"
I'll go a step further: how can we trust centralized bureaucracy to educate children, regulate the financial industry, or do much of anything else right, and untainted by moneyed interests?
This question lies at the heart of all of civilization. We need to ask it. We need to understand what we're asking. We need to move toward dealing with the implications.
Note: My list above may be incomplete, or I may have missed or left off citations. Due to an injury a few days ago, I've had a hard time sitting and working at my desk with focus. If you have an additional point or link that belongs, do not hesitate to suggest it and I may add it. I'm happy to crowdsource!
Sorry for the multiple edits. I always forget how finicky substack gets (understandably) when I copy over enumerated points with images.
Great and scary post. Your question at the end is what has been haunting me for almost 2 years. How can we trust anyone in power ever again? They knowingly lied and are still lying about poisoning us all. Then you start rewinding history and realize that they have been lying to us for decades about everything.