


Vaccine Wars Part I: What are the Risks of the COVID-19 Vaccines? (1 of 2)
The Chloroquine Wars Part XVI

"The word 'bipartisan' means some larger-than-usual deception is being carried out." -George Carlin
Before getting into the meat of this article, I want to mention that I had a hard time between starting a new "Vaccine Wars" series and including such articles in The Chloroquine Wars. But the topics branch and intersect so chaotically that it seems best to use The Chloroquine Wars as an umbrella for most all serious discussion surrounding the SARS-CoV-2/COVID-19 pandemic.
Second, I would like all readers to understand that my research on vaccines is not nearly as deep as for the drugs I have primarily written about---chloroquine and hydroxychloroquine. However, over the past few weeks I have been catching up while having nearly daily communication with a vaccine manufacturer. As such, I make no claim that the list of risks I present here is complete, that I fully understand the implications, or that my own thoughts will not evolve [more than usual]. But I wanted to have this "conversation" at a time when I see a steep number of narcissistic and strawman-ish conversations online that seem designed to dismiss the notion that the risks are worth talking about. During a large scale change in health policy that involves a new technology, that direction of conversation is not simply irresponsible, but potentially fatal and on a level with broad, existential consequences.
Next, it is worth mentioning that nobody in public health policy, nor the pundits, many of whom seem to be more narcissistic than ever before in their presentation of confidence, has offered anything that strikes me as even a basic cost-benefit analysis (CBA) of the mass vaccination programs underway, including the handful of pundit economists who vaguely refer to their CBA without ever actually offering more than a couple of mumbled paragraphs (*cough* Marginal Revolution *cough*) that seem intended to look authoritative while leaving out any real breakdown of risk analysis. If I am wrong about this observation, please send me the appropriate links, but having asked for such a CBA from scientists, economists, and public health officials, and been given nothing more affirming than a statement that such a CBA exists with a hand-wavy explanation of what it would say if it existed, I have great doubts that the discussion is much more than smoke and mirrors.

This is perhaps around my dozen-th public request for a CBA in various media formats. At the very least, we need to have the conversation about how the CBA warps across age groups rapidly given that the effects of COVID-19 rise exponentially into the elderly population. Before we poke holes in young people with vaccines, including new mRNA technology with a sparse and shaky track record (and so many unanswered questions), we should understand the cost and benefit calculi---particularly since influenza kills more Americans under the age of 25 annually than did COVID-19 in 2020.
Such a CBA begins with a summary of risks and benefits (see my approach to a CBA for the proposition early treatment with HCQ, which is incomplete on a full economic scale, but establishes a threshold for determining a likely [very] positive CBA). Those risks and benefits can be hard to weigh against one another at times, but if public policy is based on anything responsible, it is in these attempts. Of course, we should also be considerate of improvements to proposed policy, including Pareto optimization. Every action has opportunity costs associated with discarding alternatives. At times, tunnel vision can lead us to ignore the exploration of alternatives.
Before I summarize the risks that I know about, it should be noted that there are generally known risks (short term adverse events), known unknowns (like not even knowing exactly which cells in the human body the vaccines reach) among risks, and then the unknown unknowns. Even the known risks can be challenging to analyze at times, and the known unknowns more challenging. At the level of the unknown unknowns, it is responsible to analyze worst case scenarios to establish something that functions like a wide confidence interval in the result.
Now, let us examine a first order list of the risks. For the moment, I will take the extraordinary step of assuming that all the evidence is as it has been presented, despite the many general problems of corruption I have noted in previous articles, not to mention cases that the harms of the vaccines are far larger than we have been led to believe that I have not have time to read through. Note, I may edit this post later, but will tag the addendums.
Side effects/Adverse events.
This is the simplest set of risks to discuss, though even this aspect of risk analysis has been widely politicized and perhaps never fully assessed. The task of analyzing the adverse events (AEs) gets challenging when you realize that there are over 200 vaccines either approved for COVID-19 or in various stages of development. A distinct CBA should be required for each. Why is that so hard (to require of the manufacturers if not public health officials)?
For the moment, let us focus in on the Pfizer vaccine since we have a 53-page summary (without a CBA, ahem) that propelled its widespread use (already exceeding 100 million doses). A doctor I know called the AE profile of this vaccine "the worst I've ever seen".
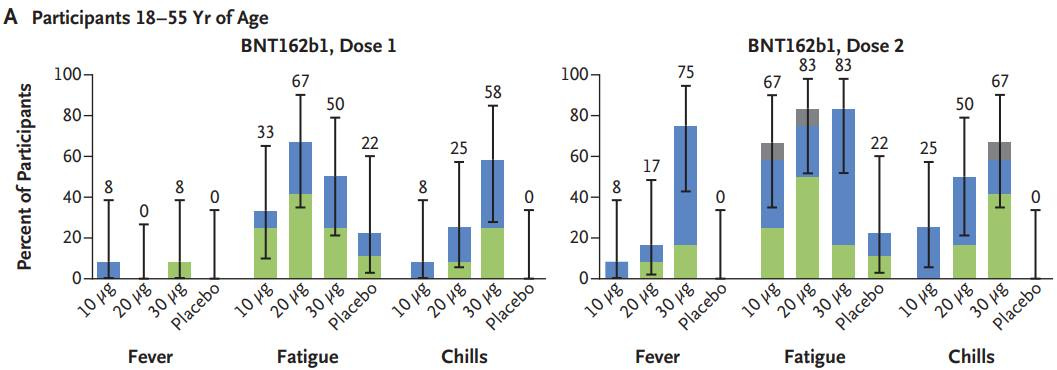
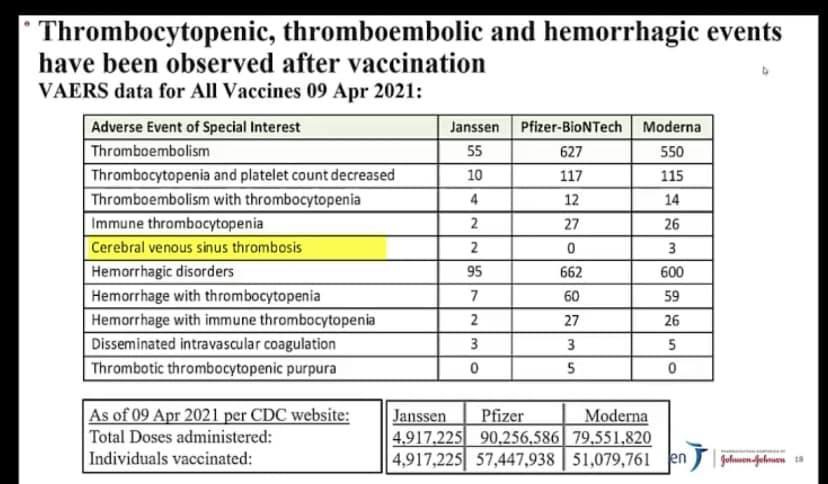
It has been reported that side effects from this vaccine often feel like a "severe hangover". We might suggest a calculus of "one day of life lost" for such adverse events. However, there are more serious adverse events such as blood clots that can be quite deadly.
There is no method we can employ to weigh "days of life lost" to various forms of suffering aside from examining the ways in which people make choices given the opportunity. Economists sometimes then jump in to attach dollar amounts. We leave a complete CBA for another time, but let us at least estimate days of life cost vs. gained. This is already hard given the amount of withheld data from the trials (raw data will apparently be released sometime next year after the vaccines have been widely delivered). While we are given numbers of COVID-19 cases 14 days after vaccination, we cannot compute the number of lives lost in each arm without this level of data.
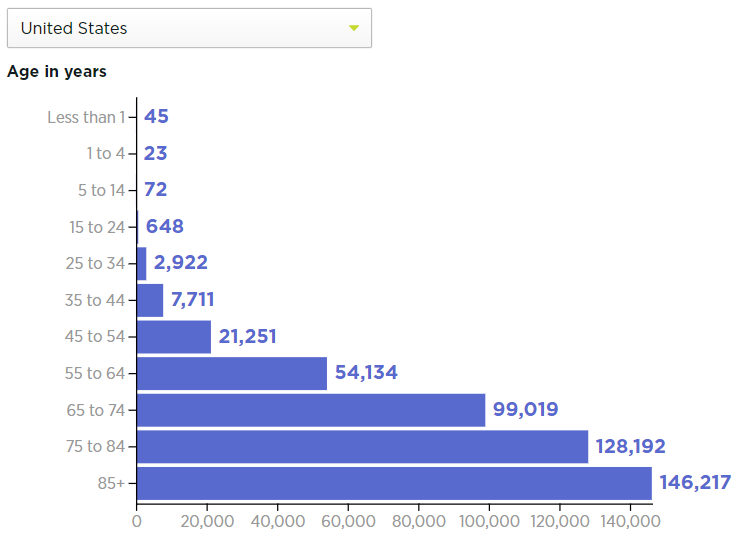
The VAERS deaths seem to have a similar age-skew as the fatalities caused by the disease itself. While I have seen lower numbers, let us assume that 16 years is the average number of years lost per death, which is a bit under 6,000 days of life lost. Next, if non-fatal adverse events result on average in 2 days of life lost per vaccinated person, that is equivalent to 5475 years of life lost per 1,000,000 vaccinated, or the equivalent of 342 lives lost per million vaccinated. Add that to the 20 deaths per million in VAERS reports (plus or minus whatever debate you might have over what these numbers represent), and the vaccines need to reduce future deaths per million by around 362 just to pull even in a CBA. That number is already more than the mortality rates experienced by the majority of all nations in the world during the pandemic. More than 100,000 lives would need to be saved in the U.S., at a minimum, to justify the side effects only. Of course, that doesn't count the costs (in human work hours, which equates to life on some level) or the remaining risks.
No, I don't know how accurate is the assumption of "2 days of life lost per jab" to headaches, fatigue, rashes, bell's palsy, and blood clots. But I've provided an anchor to the start of a conversation that never took place, but should have.
2. Disinfectants.
Okay, I'm making a joke here. But for the Never Trumpers who went crazy over Trump's suggestion of putting disinfectants in the body, I feel obliged to mention that the Pfizer vaccine contains four of them: potassium chloride, monobasic potassium phosphate, dibasic sodium phosphate dihydrate, and sodium chloride (which is actually the standard precursor for bleach). But really, such disinfectants are present in all vaccines.
3. Antibody-dependent Enhancement (ADE)
Antibody-dependent enhancement (ADE) of viruses occur when viruses "outmaneuver" immune responses, perhaps taking rides on macrophages to reach and infect new cells, then replicate more. This risk should be understood, but is less prone to coronaviruses than others in which the effect has been seen in response to vaccination or other treatment.
4. Dependence.
So far, popular vaccines do not seem to be resulting in much T cell immunity: just 31% among those who receive the AstraZeneca vaccine and 12% among those who receive the Pfizer vaccine. These vaccines seem to depend on B cell antibody emission to fight COVID-19. Antibodies aren't nearly as long lived as T cells, the latter of which may be more responsible for immunity to SARS-CoV-2 in particular (also here).
We are already being told that a third dose is in the works for those willing to receive the COVID-19 vaccines. If we forego natural herd immunity, with longer-lived T cells, we may be looking at an expensive and dangerous future of continued jabs.
So, how much do you trust the pharmaceutical companies as a life partner?
Pfizer ranks last in reputation out of these 17 large pharmaceutical manufacturers.
Pfizer ranks last in reputation out of these 22 large pharmaceutical manufacturers.
Search "Pfizer history of fines" and you will find scores of scandals ranging from bribery to illegal claims about its drugs that will take hours to read, mixed in with a handful of what appear to be public relations pieces (if you scroll that far).
Moderna is a brand new company with essentially no product reputation (outside of DARPA). But they do have a soaring stock price to justify.

Finally, it may be worth understanding that the entire business model of the pharmaceutical industry looks to be in "terminal decline".

It is no wonder that the pharmaceutical industry's lobbying arm, the world's largest, grew so much in 2020. Does it make you feel better sleeping at night to know that Pfizer has been strong-arming other nations to put up collateral that represents national defense and security to pay for legal liability of their COVID-19 vaccine?
5. Efficacy in stopping viral spread and disease.
This one seems hard to evaluate in terms of impact. There are knowns, known unknowns, and unknown unknowns all lurking right here.
First, it should be understood that the design of the trials for COVID-19 vaccines took a highly nonstandard approach, testing for disease state, not the ability to inhibit infectivity. Taking a closer look at Pfizer's report reveals that thousands of trial participants had suspected, but unconfirmed cases of COVID-19 that make the claimed 95% efficacy rate look like a joke.
Pfizer vaccine defenders seem glued to the narrative that all that matters is what takes place after day 14 when antibodies reach a protective level. But this is nonsensical logic given that nobody can skip days 0 through 14. Not only that, but the lopsided data exclusions on page 18 completely overwhelm the effect size in the final analysis. Without release of their raw data, it is impossible to make sense of the claimed calculations.

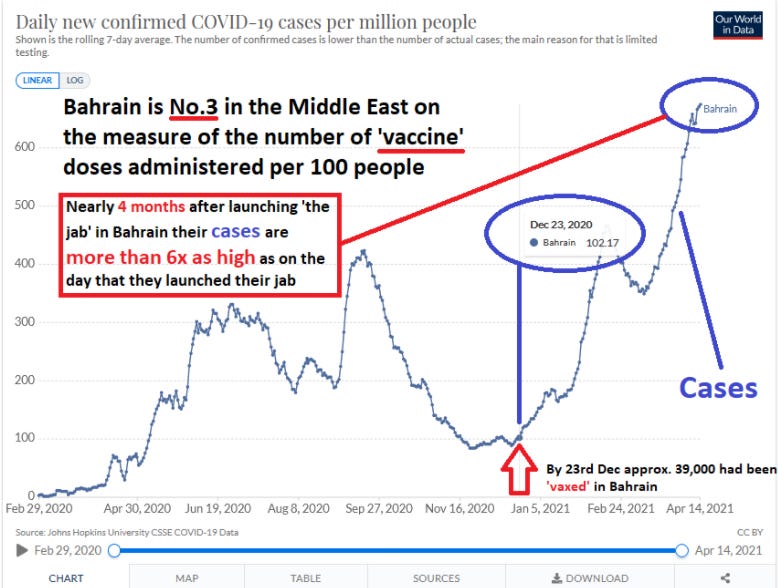
On March 18, Forbes noted that SARS-CoV-2 seems to be spreading faster in states with higher vaccination rates.
Stopping or dampening the disease state is important in a CBA, but the rate of infectivity could be more important as I point out later (see point 8).
Aside from these concerns over efficacy, it should be noted that quality control problems have also been an issue at times.
This post was too long for substack. To be continued…