


Silent Type II COVID-19?
The Chloroquine Wars Part XXXV

"I decided it is better to scream. Silence is the real crime against humanity." -Nadezhda Mandelstam
The more I read, the more I prefer my idea of redefining COVID-19 into two types, even if it takes time for physicians and researchers to get a grip on which is which with some patients:
Type I COVID-19: The collection of effects and symptoms usually associated with coronaviruses, which include the common cold symptoms and some of the symptoms associated with respiratory infection.
Type II COVID-19: The collection of symptoms associated with the spike protein. This includes perhaps the microthrombosis and blood clotting issues, some of the observed tissue inflammation, and may include symptoms caused by other pathogens that cross the blood-brain barrier which may be responsible for most or all of the neurological symptoms.

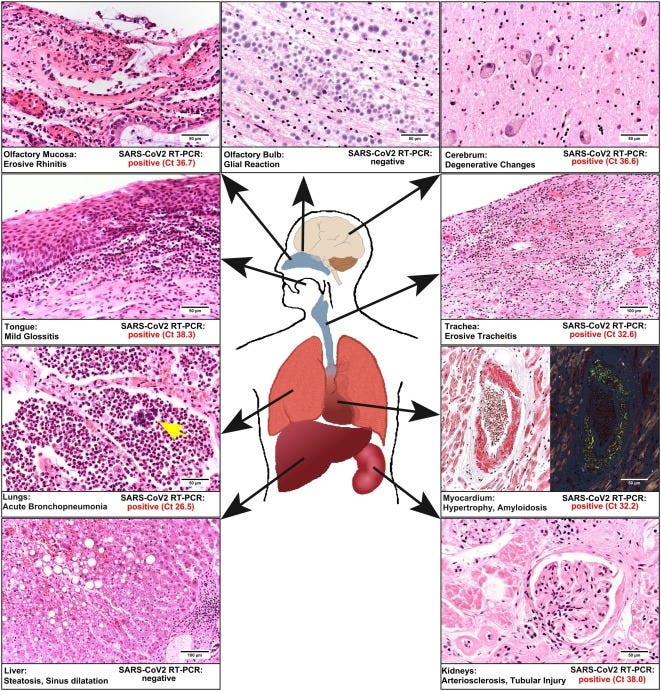
Tonight, and for the second time, I read through the first case of postmortem study in a patient vaccinated against SARS-CoV-2. After receiving the Pfizer (mRNA) injection a few weeks prior, an 86-year-old man became infected with the SARS-CoV-2 virus. From the abstract:
Although he did not present with any COVID-19-specific symptoms, he tested positive for SARS-CoV-2 before he died. Spike protein (S1) antigen-binding showed significant levels for immunoglobulin (Ig) G, while nucleocapsid IgG/IgM was not elicited. Acute bronchopneumonia and tubular failure were assigned as the cause of death at autopsy; however, we did not observe any characteristic morphological features of COVID-19. Postmortem molecular mapping by real-time polymerase chain reaction revealed relevant SARS-CoV-2 cycle threshold values in all organs examined (oropharynx, olfactory mucosa, trachea, lungs, heart, kidney and cerebrum) except for the liver and olfactory bulb. These results might suggest that the first vaccination induces immunogenicity but not sterile immunity.
I'm not a doctor and won't play one on substack, but I'm trying to make as best sense of this as I can. The patient had an immunogenic response due to the vaccine, meaning that his immune system did react as a result of the injection. However, he was able to catch COVID-19 (no sterile immunity). Eighteen days after receiving the mRNA injection, the man was hospitalized for worsening diarrhea, but tested negative on both SARS-CoV-2 antigen and PCR tests.
Day 23: Patient shows elevation in C-reactive protein, indicating inflammation.
Day 24: Another patient in the man's hospital room tests positive for SARS-CoV-2.
Day 25: The patient himself tests positive for SARS-CoV-2 via a low cycle threshold PCR, which indicates a high viral load (it takes over 130,000 times the viral load to test positive at 28 cycles as it does to test positive at 45 cycles, the latter of which was the cutoff for testing in this case).
Day 26: The patient expires.
The evidence suggests the patient contracted the virus from his hospital roommate. Once exposed, the virus, which has an average incubation period of just over 5 days, rapidly ramped up in his system despite the presence of spike protein-specific antibodies. Here is the scary part: postmortem analysis revealed SARS-CoV-2 in organs all over the man's body, including in his brain (pictures below from the paper):
Can we say that COVID-19 contributed to the man's demise? Again from the study:
We did not observe any characteristic morphological features of COVID-19 reported in comprehensive morphological autopsy studies so far (Schaller et al., 2020, Edler et al., 2020, Ackermann et al., 2020). We did not find any typical signs of diffuse alveolar damage in the lungs, but we identified extensive acute bronchopneumonia, possibly of bacterial origin. We concluded that the patient died from bronchopneumonia and acute renal failure.
I don't know how to answer the question of cause of death beyond trusting the opinions of the authors except to say that any damage caused by SARS-CoV-2 infection could not have helped this already sick man. More interesting (if I can use that word here) might be to imagine how the damage caused by this vast viral infection, including that caused by the spike protein (which is itself cytotoxic and opens the blood-brain barrier), might have progressed in a healthier patient.

The condition of silent hypoxia (or "happy hypoxia") describes some COVID-19 sufferers who present no outward symptoms at all until they find themselves struggling to breathe, with low blood-oxygen. The lack of a signal associated with any illness means any potential treatment could come too late.
Silent Type II COVID-19?
Now let us ask the important question:
Is there some mechanism by which the mRNA injection might have silenced symptoms while allowing SARS-CoV-2 (and the spike protein) to permeate the man's body?
Put differently: could mRNA injections (or possibly other vaccines) induce silent Type II COVID-19? Follow ups:
If so, is this case anomalous (though it just so happened to be the first such postmortem analysis)?
If this case is not anomalous, what are the characteristics of patients who might suffer or die from silent Type II COVID-19?
How numerous might such a population be?
Could silent Type II COVID-19 be already developing at an albeit slower pace in healthier populations not hospitalized with already serious conditions?
Will winding the PCR cycle threshold for breakthrough cases down to 28 result in millions of people experiencing silent Type II COVID-19?
Aside from any other controversies over deaths, blood clots, myocarditis, or other serious adverse events, might it be the case that mRNA injections could be seeding a Type II COVID-19 epidemic that could play out over coming months or years among millions of recipients?
Such a question, which might have a simple answer for all I know (though I haven't seen anyone address it), is the kind of question that makes a rushed mass-scale experiment seem unwise. It may be better to hear COVID-19 scream than to suffer its silence.
Type II comes later, when the immune system kicks in. Clotting is caused by the antibodies produced against platelet factor 4: https://www.nature.com/articles/s41586-021-03744-4 (the study is about vaccine induced clotting, but the real virus triggers the creation of these antibodies too). Additionally, the virus destroys ACE2, ACE to is also an enzyme that creates stuff that reduces oxidative stress, oxidative stress in the blood vessels raises the clotting factors. Silencing the immune reaction is done by the virus itself, it sends proteins into the nucleus that dampen the gene expression needed by the cell to produce stuff for self defence and to alert the immune system (ivermectin stops the virus from doing that).
From a data science, mathematician and computational economics standpoint, very little if any of the reporting on covid-19 since 2020 is meaningful or can be trusted.
The PCR tests in so far as the cycle thresholds being set to numbers above 28 amount to exploitation parameter setting in algorithms such as reinforcement learning that result in model over fitting. Therefore what you end up with are a lot of false positives and false negatives.
What makes the PCR testing even more problematic is the asymmetric testing that was happening once the vaccines started being rolled out, i.e. vaxxinated tested at thresholds of 28 while unvaccinated tested at a threshold of 45.
Therefore, not only do we not know if all the cases and deaths up until now have truly been covid or regular flu or cold. Compounding this is the decision to count everything as covid, so death with a positive covid test was counted as death from covid even if covid was clearly not the cause of death reported by the doctors.
The abnormal nature of contracts allegedly signed with the pharma companies in relation to the vaccines (such as IP protection and using military bases as collateral to fund vaccine purchases, etc) raises further questions around perverse incentives just as hospitals being paid per covid case and death reported.
The handling of the SARS-Cov2 outbreak has been beyond moronic from the get go and it continues to be as the various vultures circle. One could understand early on when no one knew what we were dealing with, but 18 months on and nothing has changed but things have become more entrenched. So while it would be welcome to see a stop to the mass vaccinations during an pandemic entailing a family of viruses known for their mutations, I am not convinced the insanity is going to end any time soon. Far too many financial and other interests (including pride and egos) at play it seems