

Are UK's Vaccinated Dying More from the Delta Variant? Part 2
The Chloroquine Wars Part XXXVIII

A few days ago I worked up a spreadsheet for the purpose of first order analysis of vaccination efficacy data and study of the Delta variant as per the reports coming out of the UK. A friend suggested that I keep up with the reporting, which is mostly a matter of making a new tab in the spreadsheet and updating the numbers from the latest PHE report, then adjusting a few parameters (recent vaccination rate) and variables that aren't provided by the PHE (within ranges that make sense). It will be interesting to see if my results prove to be consistent. As it turns out, the PHE computed very similar relative reduction rates for both 1 and 2 doses as those I stated were my "best guess" in my prior article.
Since without a true risk curve I was forced into broad risk grouping with some guessed variables, I'm pleasantly surprised---particularly given the ratio between these numbers, which surprised me a bit given that the relative reductions in mortality are far closer than those of case numbers. So, if these numbers hold up, we might say that the second jab appears to stifle a wide swath of mild to moderate cases, but doesn't give any extra protection to those destined for the worst outcomes.
On to this week's numbers!
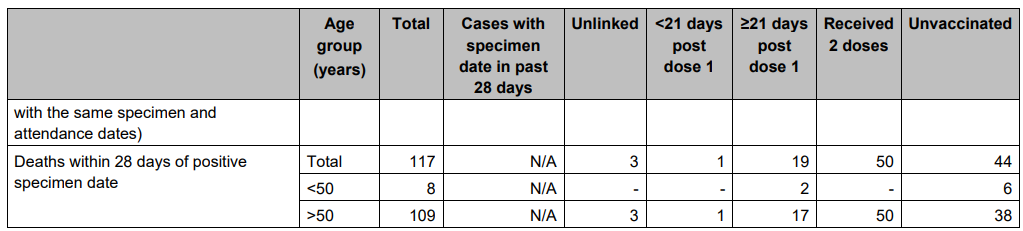
I went ahead and started with the assumption of 60% vaccinated with respect to this data. The total vaccinated population is slightly higher, but some data predates some vaccinations, presumably. Fortunately, we don't have to get into extremely complicated estimations because the Delta wave is almost entirely recent. If you want to know more about the methodology I'm employing, please read the last UK data article.
I will stick to the same 5 examples as last time, with tiny adjustments that fit the growing vaccination rate. Example 1 is what I consider a highly reasonable set of guesses as to the same six variables as last time:

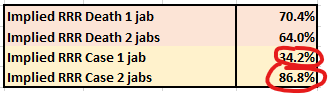
The relative risk reductions (RRRs) for 1 and 2 jabs look slightly better than last time, but the vaccine efficacy in stopping mortality looks a little worse than last time (70.7% and 63.6% RRR). Notice that the Delta variant looks to be 90.6% less deadly in this case output. That's great news!
I've added some columns to my analysis:
ICR = Implied number of COVID-19 cases avoided.
ICR/(M)Jab = Implied number of COVID-19 cases avoided per million vaccine doses.
ILS = Implied number of COVID-19 deaths avoided.
ILS/(M)Jab = Implied number of COVID-19 deaths avoided per million vaccine doses.
NNV represents the number of doses needed to reduce the number of cases of COVID-19 by 1.
Notice that the second jab does not seem to reduce mortality as much as the first:
2*1.86 - 2.78 = 0.94 deaths avoided per million second-doses.
This observation may become important in the debate over whether additional doses beyond the first achieve a positive risk-benefit. The answer may come down to the subgroup. I personally doubt there could be positive risk-benefit for those outside of high risk groups, but I will lay out that case more completely in another article.
Example 2: Adjusting the variables, mostly to push more prior deaths from the high risk group to the low risk group while mildly moving assumed vaccination proportions results in a lower implied RRR with respect to mortality:

Example 3: Within the realm of the worst case scenario for the vaccines:

Under the inputs used to generate Example 3, not only does the first jab increase mortality, but the Delta variant is 95% less deadly per case than during the previous UK infection wave.
Example 4: Within the realm of the best case scenario for the vaccines:

Here, the second jab saves a lot more lives than the first (10.21 per million doses).
Example 5: Back to something I consider more realistic for all the reasons I mentioned in the last article:

Remember that without a real risk curve to work with, it is hard to pin down actual numbers, but the case RRR numbers are consistent across two weeks, five sets of variables each, and also with the PHE's computations. This seems suggestive that these computations are within the realm of reason. I still disagree with those who say that the vaccinations are making people die more often of COVID-19.
More importantly, I also still disagree with the mass vaccination program. In particular, nearly all lives saved are in the high risk group. While vaccinating those in the low risk group might decrease spread into the high risk group, that's asking young healthy people to act as human shields. I also believe that when the vaccine deaths and adverse events are finally tallied and compared to either a ring vaccination strategy or combination ring vaccination and early treatment strategy, the current plan will look quite foolish and possibly even nefarious.
Nefarious has a ring to it.
Hi Michael,
I only recently found your site, it's got a lot of great analysis.
I wondered if you have looked at the more recent UK vaccine surveillance files?
Starting I think around week 36 they began reporting rates per 100K population (there are also time series of vaccination rates broken down by age).
Anyway, a strange phenomenon has arisen where case rates are higher among the vaccinated population, although hospitalization and death still appears at lower rates.
Week over week, the difference in case rates has continued to get worse for some months now.
I'm really not sure what to make of it, and wondered if you had seen it or written about it?
One possible theory is that the delta variant finds more fertile ground in vaccinated populations due to the fact that it evades the NTD antibodies produced by the vaccine.. but perhaps delta did not seem generally more adaptive (and therefore did not spread widely) in largely unvaccinated populations?
See these for more discussion of evolution of delta and vaccine evasion:
https://eugyppius.substack.com/p/the-mystery-of-the-variants
https://eugyppius.substack.com/p/preprint-the-sars-cov-2-delta-variant
Thank you so much for all your hard work!
You are keeping many people slightly more sane (by some metrics).