


The Meta-Analytical Fixers, Part II: Public Servants or Middling Saboteurs?
The Chloroquine Wars Part LXXVII

I don't have time for this level of garbage, so I won't spend much on it, but something needs to be said. The propagandists vastly outnumber the people of good faith in The Chloroquine Wars, if that is now my general term for this medical authoritarian battle.
I've been forwarded this BBC article multiple times.

It's interesting to see how the BBC presents Gideon "Health Nerd" Meyerowitz-Katz, Kyle Sheldrick, Nick Brown, and James Heathers as something like a team of COVID Superfriends, taking down COVID disinformation, though without anything like a track record to talk about. For instance, when I asked Health Nerd and Sheldrick each about this error-laden meta-analysis claiming a lack of ivermectin (IVM) efficacy, neither had much to say (IIRC, they simply did not respond, though I blocked Sheldrick on Twitter for what I felt was harassment a short time later).
Dr Kyle Sheldrick, one of the group investigating the studies, said they had not found "a single clinical trial" claiming to show that ivermectin prevented Covid deaths that did not contain "either obvious signs of fabrication or errors so critical they invalidate the study".
But the team of COVID Superfriends does have one notch in their belt. Maybe. In a high profile case, some of the COVID Superfriends found extremely obvious flaws in the claimed raw data of a now-retracted paper. The author claims that the data set is not his, and that he will challenge the retraction. The whole story seems fishy to me to the extent that it strikes me as entirely bizarre and unique that such obviously faked lines of data would even exist in a sharable form, much less be shared given that researchers have no requirement to share their data. Also, it seems giggle-worthy that it would take more than one of them to perform that task, but hey, people need friends to push forward with their work sometimes. It would be hard for me to look into the story closer than that.
At this point, I'll note that Brown and Heathers are "famous" for inventing the GRIM test, which is something like an error-checking method you might teach middle school students, and that most any competent statistician with number sense does instinctively, but sadly sometimes applies to actually published research. But to be fair, much of the time it applies, it likely represents something simple like researchers adding or removing a data point [appropriately] while forgetting to update the computation on their spreadsheet because one person in the lab didn't realize the other person didn't automate the computation (I've personally caught such errors, reported them to researchers, and been thanked for it). This is, in fact, exactly the kind of error Health Nerd and Sheldrick raved over when I discussed the "horrid IVM research" with them online. They seemed emotionally unable to let go of any sort of notion that before making damning statements about researchers---working in nations with access to fewer trained biostatisticians---and their results, it might be polite and reasonable to just email them about the problem. Heck, sometimes we just fix that stuff in preprint. Yawn.
I will also note that Heathers stands out as less-than-objective in my mind after this apology piece over The Lancet's publication of the Surgisphere paper. If asked to defend my downgrading of Heathers' objectivity on this level, I would simply refer to my remarks about standards here. If database readouts are not going to ever be checked on the simplest level, including by people in the field who might be able to ferret out phony data or apply a basic sniff test (which Surgisphere clearly did not pass), what the hell is the point of peer review? Under such standards, scientific publication is no longer able to make any judgments, and the process becomes a money-driven battleground.
Too late?
Now, where to begin with regards to the entirely demolished IVM research pool, as the COVID Disinformation Superfriends would have us see it?

It sounds like Team COVID Disinformation Superfriends state that they can point out flaws in two or four or six of the studies? I'll let Computer Scientist Alexandros Marinos explain.

Aside from all the many good points Alexandros makes, the central thesis of the article is entirely rhetorical. There is an incorrect implication that randomized control trials are the only studies worth examining, which is a claim few statisticians agree with (here and here), all of whom seem to work in or for the pharmaceutical industry (including the media-pharmaceutical complex). There is also the implication that "to show that ivermectin prevented Covid deaths" means "achieved a statistical significant threshold of p < .05" without any kind of further discussion of trial powering, grouping, or the fact that Ronald Fisher, the statistician who invented the methods of inferential statistics used to measure such results, openly and adamantly disagreed with such rhetorical use of statistics.
It's sad and disturbing how so many doctors don't understand the history behind the forms of pseudo-statistical brainwashing they're fed in order to capture them into reading medical research statistics like code to be injected into their brains, but that's another story for another day.
A few weeks ago I tangled with Health Nerd on Twitter, not knowing anything about him except that he wrote an almost entirely incomprehensibly incorrect thread about statistics of ivermectin studies.


The most amazing part was when, backed into a corner of impossible defense, he claimed that there is no such thing as a study confounder local to a single study in a research pool. In other words, all study confounders are necessary global! And when offered the chance to convince me of that on camera, he dodged. Then he and Sheldrick went on an absurd campaign to state publicly as many times as possible that it was me who dodged, but I'm happy for as many people as would like to read the thread and decide. Yawn.
It will be interesting to keep an eye on his team of Superfriends to count the number of confounders they spot in one, but not all of the studies.
Remember the Fake Oklahoma Story of Ivermectin Patients Flooding Hospitals?

That story was quickly unraveled by numerous people.

Further demonstrating his clear good faith in checking the evidence, Health Nerd was among those completely drawn into the medical-partisan warfare over the strange tale of IVM overdoses filling ER rooms in Oklahoma. I kept wondering who would even believe such a story, but this answers that question.
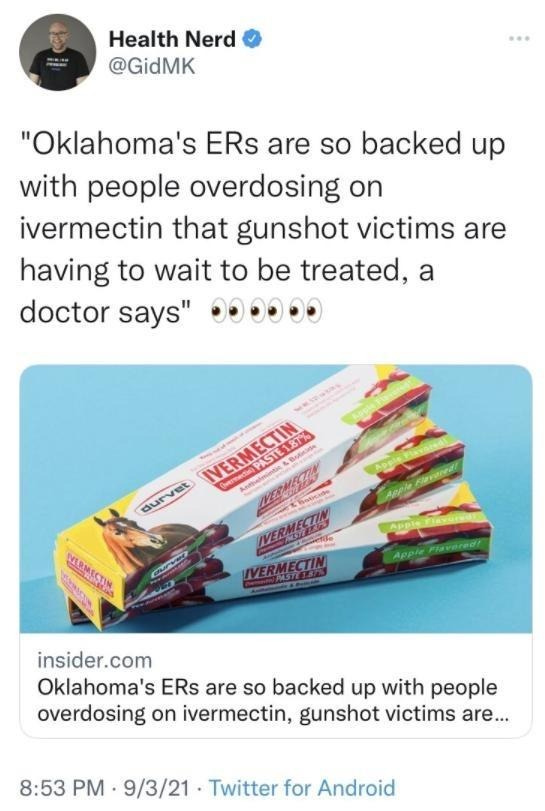
If you're looking for some way to understand the BBC's level of credibility in all this, take a look at how the BBC handles the IVM overdose story in their "superfriends take down ivermectin studies" article. The article mentions, without noting the way Health Nerd helped push that false narrative, that increases in poison control calls over ivermectin never amounted to much. However, note their last sentence in this paragraph contains no citation, much less an attachment to ivermectin usage (italicized emphasis mine, only), which is to say they're ambiguously mentioning some terrible things people experience in the same paragraph without making it clear that they've researched the problem in a way that attaches these side effects to anyone's actual use of IVM.
Calls over suspected ivermectin poisonings in the US have increased a lot but from a very small base (435 to 1,143 this year) and most of these cases were not serious. Patients have had vomiting, diarrhoea, hallucinations, confusion, drowsiness and tremors.
The naked insinuation is disturbingly irresponsible, and beneath journalist ethics, or else plain stupidity. I'll let you decide. But it gets worse...
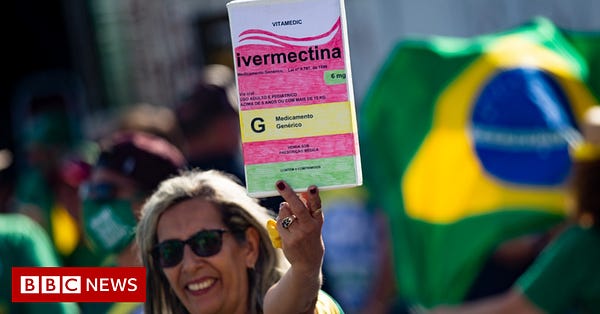
Ivermectin and Peru
Peru is one of the nations that thrust IVM into the spotlight. Sure, a handful of doctors and medical scientists were talking about it for months, including Dr. Antonio Cassio Prado, who stated last year in this video that none of the 3,000 Brazilians he gave IVM to got sick with COVID-19 in Sao Paulo---a city notably ravaged by contagion. But these stories don't get out in the media, easily. But around the middle of 2020, while suffering one of the world's worst COVID-19 outbreaks, Peru turned to IVM to bolster its treatment arsenal. As TrialSiteNews reported, Peru saw a steep drop in COVID and deaths from that point---a trend that reversed itself once Peru's new President, Francisco Sagasti, restricted the use of IVM.
Multiple research papers emerged from Peru during that time that seem to have never made it out of preprint.
Now, consider this portrayal of Peru's use of IVM by the BBC.
Dr Patricia Garcia, a public health expert in Peru, said at one stage she estimated that 14 out of every 15 patients she saw in hospital had been taking ivermectin and by the time they came in they were "really, really sick".
The BBC article also goes on to claim a co-ordinated harassment campaign of doctors who do not prescribe IVM, but provide no evidence at all to back that claim up. The vacuously presented statement follows a discussion of pro-IVM Facebook groups, so the implication seems to be that these communities are frenzied mobs, making the lives of physicians more difficult by the day during these hard times.
Back to Peru: Let's remember that Peruvian medicine is a complex machine given the way U.S. medical and intelligence authorities have participated in forced sterilization programs there. The politics in Peru involve an extremely nasty underlying battle for the future, sometimes pitting Peruvians with European ethnic roots against the native population. This means that among medical personnel, you can find those conscripted in that battle willing to say anything, particularly when paid. And while I didn't mention that while writing about The Meta-analytical Fixers (the two lead authors on those papers immigrated from Peru), it was certainly on my mind.
Maybe They're Right
For all my critique of Health Nerd's COVID Disinformation Superfriends team, I'm not entirely certain they'll be wrong. I will admit openly that I have been concerned since I discovered how the Surgisphere team posted an IVM study to preprint early during the pandemic, then later retracting it, that there might be an organized operation to produce and then dismantle fake studies with the goal of casting doubt on their efficacy. It wouldn't be the first time.
That still wouldn't tell us anything new about ivermectin's efficacy in treating COVID-19 patients.
Hi Alex, Gideon Meyerowitz-Katz has been completely unreasonably dismissive of ivermectin and vitamin D since this 2020-05-13 article: https://gidmk.medium.com/should-you-take-a-vitamin-d-supplement-for-covid-19-63d922f24953 . I have tried to engage him in discussion in various ways since then and nothing comes back.
The Guardian publishes his writings as if he is both an expert in the field and as if his perspective on such matters is all that is required to settle a question.
I am wary of criticising people in potentially public spaces, not least due to the potential legal repercussions. If I had anything positive to say about GMK I would say it here. I have nothing to say in this regard.
There are numerous noisy people who think themselves experts, who are frequently regarded as experts, and who may indeed be experts in all the relevant fields who complain about genuine good evidence (in my opinion) for the importance of vitamin D for the immune system, and/or for the safety and effectiveness of ivermectin as an early treatment for COVID-19. Their standard approach is some mixture of:
1 - Never actually mentioning or criticising the best evidence for the effectiveness of the nutrient or drug.
2 - Picking some weak or suspect study, pointing out its errors (perhaps unreasonably) and then portraying this as the best evidence, or representative of the best evidence, for the nutrient or drug.
3 - Portraying extreme resistance to new information as a virtue. This is usually in the form of insisting on RCTs, ideally not in third-world / developing countries, each showing splendidly positive results, to be covered by at least one and ideally more resoundingly positive meta-analyses.
There are good reasons for proposed new medical treatments need to surmount such hurdles before being widely implemented outside clinical trials - when the treatment is a new drug, where the safety is not known and is in fact difficult or impossible to research in the absence of millions of people having been given the drug over many years.
However, it is a mistake to insist on such high hurdles, which would take years and tens of millions of dollars to overcome, in the middle of a crisis, for very well researched nutrients such as vitamin D3 (or calcifediol, which what all immune cells need 50ng/ml of, and which is produced over days from D3 by hydroxylation in the liver), for a very well tested drug such as ivermectin, or for a very well researched and widely used (without prescription in the USA) hormone such as melatonin: https://c19melatonin.com.
The question of why so many physicians, immunologists etc. are so clueless about vitamin D is the most complex, perplexing, difficult and important problem I have ever encountered. One day I will write lots about it at https://nutritionmatters.substack.com .
Doctor's face extreme difficulties with the amount of knowledge and experience they are supposed to bring to bear on every clinical decision, often based on limited time and limited information. They can say X, have it misinterpreted as Y, and have Y cause harm or death to their patient or to someone else. They are very wary about changing their beliefs and are highly resistant to anyone pestering them to do so.
However, this whole global disaster would not be occurring at all if most people's 25-hydroxyvitamin D levels were 50ng/ml (125nmol/L) or more. Doctors, collectively, could have and should have recognised the need for this over ten years ago. There's a chance that in that time, they could have convinced many or most people to supplement D3 to attain this. Then SARS-CoV-2 R0 rates would generally be below 1.0, there would be no pandemic, and very few people with such good 25-hydroxyvitamin D levels would be seriously ill, even without early treatment or vaccination.
They haven't recognised this, for a variety of reasons, and this is a single point of failure for all humanity, apart from a few people who have figured out the need for good D3 supplementation, or who have been advised to do so by their doctor or nutritionist. But every single person is trapped in the global disaster of the pandemic's direct effects and the effects of the numerous attempts (lockdowns, vaccines - but little or nothing in terms of nutrition or early treatment) to control it.
Returning to ivermectin, the question is not whether there are X number of glowing RCTs and Y number of positive meta-analyses, all served up in the manner to which some people have become accustomed. The question is whether it is a safe and effective treatment for COVID-19. This question can be converted into: 'How could it be unsafe and/or ineffective in a world in which the best available trials which seem to show its effectiveness actually exist?" Since it is not possible for all those research articles to be totally or even largely faked, a proper line if enquiry leads to scrutiny of the 7 most significant Early Treatment RCTs listed in the "after exclusions" table at https://ivmmeta.com .
Click on the left column for the studies named Espita-Hernandez, Bukhari, Elalfy, Mouyra, Merino, Faisal and Aref. There you will find links to the articles and the anonymous ivmeta.com people's assessment of these studies.
Don't complain about some being preprints or being in journals not indexed in PubMed. Don't complain about them not being done in Western nations. Be glad that some MDs and other researchers have gone to the trouble of conducting these RCTs, including knowingly harming and killing some of their patients in the control arms, for the benefit of people like us who keep asking for more and more evidence.
Also have a look at their assessment of the trials with red boxes on the right, Krolewiecki (non-significant negative results, somewhat significant positive result), Vallejos (similar, low risk patients, potential difficulty excluding patients who had not already used ivermectin) and Buonfrate (too late).
Don't complain about obviously professional meta-analysis work being done anonymously - these people need to earn a living.
Now, what is the chance, given the existence of these studies, that ivermectin is either unsafe or ineffective for early treatment of COVID-19? I think the chance is zero.
As far as I know, none of the noisy critics of Ivermectin deal with the best evidence like this.
My long suit is Monsanto's genetically engineered foods where Bill Gates has been a key investor and promoter of false claims and industry science that includes a vast network of front groups with media and academic shills that are featured as experts. This is more of the same.
Among the oldest and most abusive is original Big Tobacco/Petrochemical funded group ACSH who defend toxic profiteers with a stable of compromised sources. Sourcewatch has fab detail for ACSH which is worth a glance.
https://www.sourcewatch.org/index.php?title=American_Council_on_Science_and_Health
First red flag for me is Gideon Meyerowitz-Katz — January 18, 2018 featured by ACSH to defend Red Bull energy drinks. Like most food PR he references "sugar" which is not an ingredient but is used as a blanket term to included high fructose corn syrup as substantial equivalent. That's an odd oversight error for a man centered on diabetes research.
https://www.westernsydneydiabetes.com.au/about-us/the-core-team/gideon-meyerowitz-katz
Defending Red Bull against negative study results at ACSH puts Gideon in the stable of writers who also find toxins in organic baby food alarmist.
https://www.acsh.org/news/2018/01/18/red-bull-not-going-destroy-our-youth-and-kill-us-all-12437
More ACSH focus - https://www.acsh.org/news/2021/10/06/heavy-metal-tainted-baby-food-congressional-report-omits-important-science-15855
Then we have the author Jack Goodman who has a series of lies in his reporting of COVID vaccines. This piece from 2020 Covid-19: What’s the harm of ‘funny’ anti-vaccine memes?
Goodman claims safety and efficacy for vaccines that is entirely baseless putting his "science" into question. https://www.bbc.com/news/55101238.amp
"Vaccines go through rigorous safety checks before they can be administered to the public, with side effects closely monitored. Covid vaccines: Who decides if they are safe?"
This links to an opinion piece that reads like PhARMA press release. False claims aren't debunked they are advanced.
"People will still be offered the jab even if they have had Covid-19 in the past. That's because natural immunity may not be long-lived and immunisation could offer more protection."
https://www.bbc.com/news/health-55056016
Then Goodman adds "Vaccines must meet a high standard of safety and effectiveness before they are approved for use - it's misleading to call them experimental. "
Consider the source & follow the money.. his conclusion is revealing ""But the case can also be made that vaccines actually increase people's freedom to do things they otherwise wouldn't be able to, and can also contribute to safeguarding other people's personal freedoms too."
Couldn't be Bill Gates funding to media science helps bias of could it?
https://web.archive.org/web/20200414143731/https://philanthropynewsdigest.org/news/gates-foundation-awards-20-million-to-bbc-world-service-trust