


Proof of Statistical Sieves in VE Data, Part 2: ONS Data
The Vaccine Wars Part XXXVII

"And if all others accepted the lie which the Party imposed—if all records told the same tale—then the lie passed into history and became truth." -George Orwell, 1984
I may have stumbled on the exact nature of the statistical sieves in the UK data that generate a false appearance of vaccine efficacy (VE). Follow me on this journey…
In this article, I make the argument that the UK's Office for National Statistics (ONS) data strongly suggests miscategorization of COVID-19 deaths that gives a demonstrably false impression of efficacy of COVID-19 quasi-vaccines.
Late last week Steve Kirsch called me to discuss the UK's Office of National Statistics vaccination stratified data set through the end of January, 2022. He published an article about it (which includes data sources if you're interested), though I would encourage readers to see Steve's explorations as ongoing. I agree with him that there are issues with the most straight-forward view of the data. Steve and I and others are examining the data, and still learning more.
Ultimately, I have too many large scale tasks (the DMED story among them, and I'm still mortified that there is little effort to focus on it because WOW, MASS DATABASE MANIPULATION SEEMS LIKE AN IMPORTANT WEAK POINT IN THE ARMOR, HINT HINT, AND IT'S STARTING TO CREEP ME OUT THAT THOSE PURPORTING TO PUSH AGAINST THE VACCINE MANDATES AREN'T DOING ANYTHING WITH THE PLAIN OBSERVATION THAT THE DATA JUST MAGICALLY CHANGED IN THE MIDDLE OF 2021) to go deep with the ONS data. Some others have probably written some revealing articles on the ONS data. Feel free to drop the better analyses in the comments, if you have seen them. If I have the chance, I'll read them. But I do want to share some thoughts I had while examining this data that might be key to the story. Hopefully what I have to say will add to an understanding of the ONS data for at least some audience.

Data Limitations
One gripe I have with the data set is that I don't have the clean data to be able to perform the obvious risk-adjustment with. Risk-adjusted person days are the obvious appropriate step for the true evaluation of VE as I have written about before. Seeing that stripped away from raw data prior to presentation again and again is irksome, but becomes suspicious after a while. These health agencies have enormous budgets and some of the best access to statisticians in the world. Who exactly wants for me to believe this kind of work gets out of those offices without at least a discussion and an asterisk?
In examining the data, and thinking about the data limitations, I made an observation that may be key to understanding what kind of funny business is going on.
The Non-COVID Deaths Speak Again
Recall the Vaccine Safety Datalink (VSD) study that showed the vaccinated dying far less often from non-COVID illness. It amused me to see the way this implied (as in necessarily) substantial protection from homicide, suicide, and car accidents.

Stand in line for your immortality shots!
I really don't know what to say about this level of absurdity, but we need to give this effect a name in order to better convey it. And it's really just so absurd that I want to call it "the Topol effect". But Eric Topol is so absurd on so many different levels that naming it after him would result in further confusion, so I'll call it the "immortality effect".
It would be interesting to find out if there is evidence of the immortality effect in the ONS data that forces us to choose between accepting that either (1) there is a statistical sieve in play, which would carry over to vaccine efficacy (VE) computations of all forms, or (2) that the vaccines cause people to drive better, dodge bullets, and fix their lives (in addition to survivor cancer for much longer and maybe only having heart attacks in the immediate vicinity of defibrillators and EMTs). Do we see the immortality effect in the ONS data, also?
Yes! Yes, we do! And I used exclamation points because here we get a much more interesting view of what is likely to be going on with the data.

Note: I put these calculations in the hands of Steve Kirsch and also Chris Masterjohn. I don't know if they've checked my work, but it's pretty ordinary data work that involves setting up data in matrices that can be easily copied to a bunch of cells at a time.
First: The number of person-years in the youngest cohorts is not large, so that data is a bit noisy, but it is at least noteworthy that young people who get vaccinated are dying from non-COVID causes at a faster rate after getting vaccinated. This jibes with the observations of the dangers of high rates of myocarditis, pericarditis, and other ailments among young people. Add this to the negative efficacy rates of the vaccines against the recently dominant omicron strains, not to mention the tiny number of potential lives saved or improved, and the rationale for vaccinated young people gets weaker with this data set.
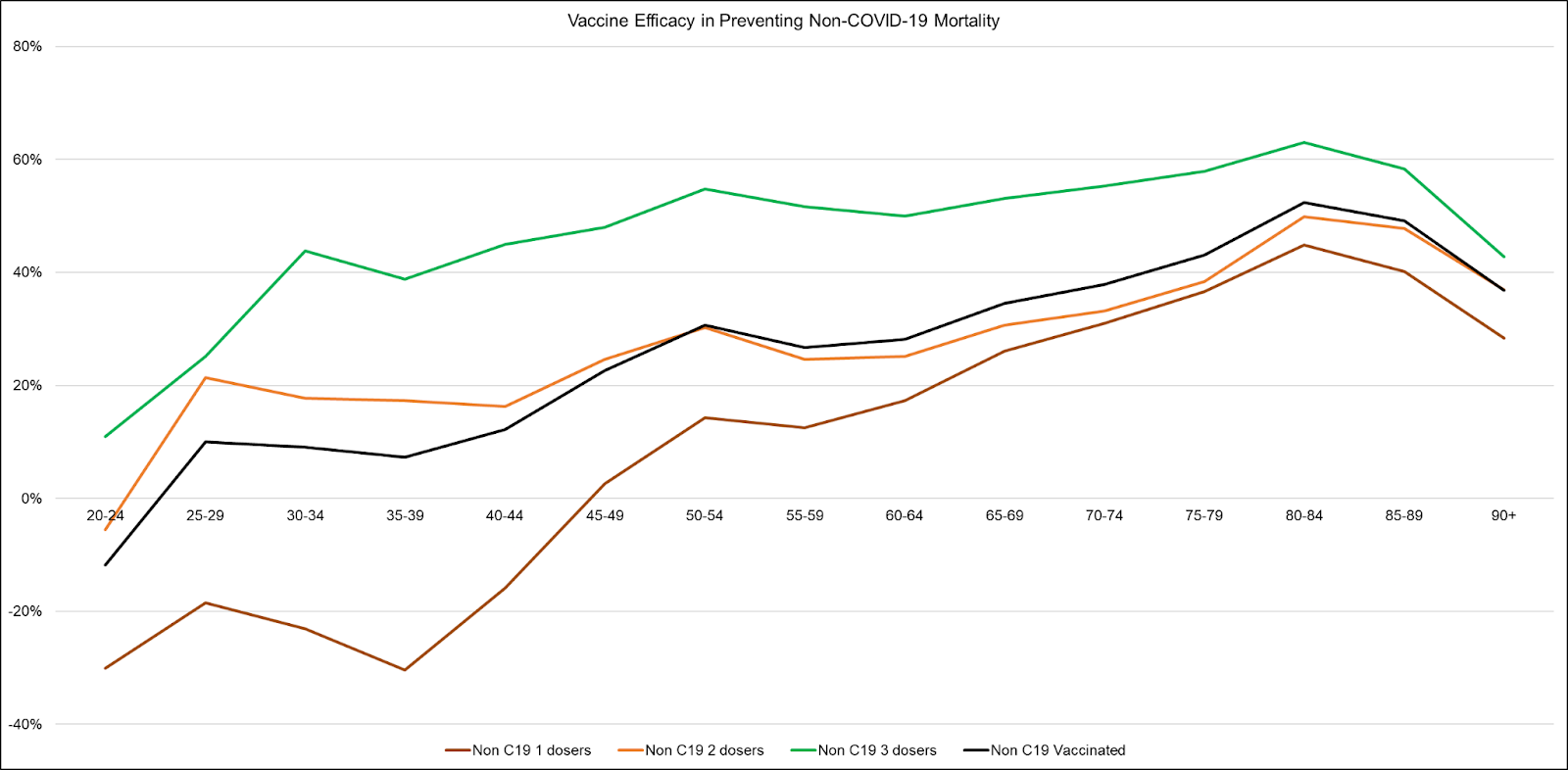
Second: In most buckets, and for most cohorts, we see substantial vaccine efficacy (VE) in the prevention of non-COVID death (the immortality effect).
Huh.
Further, this immortality effect starts small (or even negative) among young people, but grows to a substantial amount (not quite as high as the VSD numbers for most age groups, but close) for the elderly.
If this doesn't make you wonder if data is being arranged to sculpt a story, you may be stuck in a bias that's worth checking. COVID-19 vaccines are not likely helping people stave off car accidents, bullets, cancer, heart disease, or iatrogenic disease. In fact, in the case of iatrogenic disease, we should expect a lower rate among people who seek fewer medical services, which I wager includes a substantial portion of the unvaccinated.
Next, note that this supposed immortality effect…wait for it…it wanes over time!
Yeah. I know, right? If we trust what's being reported (raw data stripped away, so we're in the dark about how we got here) then the experimental injectable biological products show efficacy in preventing death from non-COVID causes and that this efficacy wanes over time. I'm trying to think of another effect that looks like that…ever in the history of biomedical research…I just can't think of…OH, that's JUST LIKE the supposed VE of these same products in preventing COVID-19 mortality.
Huh.
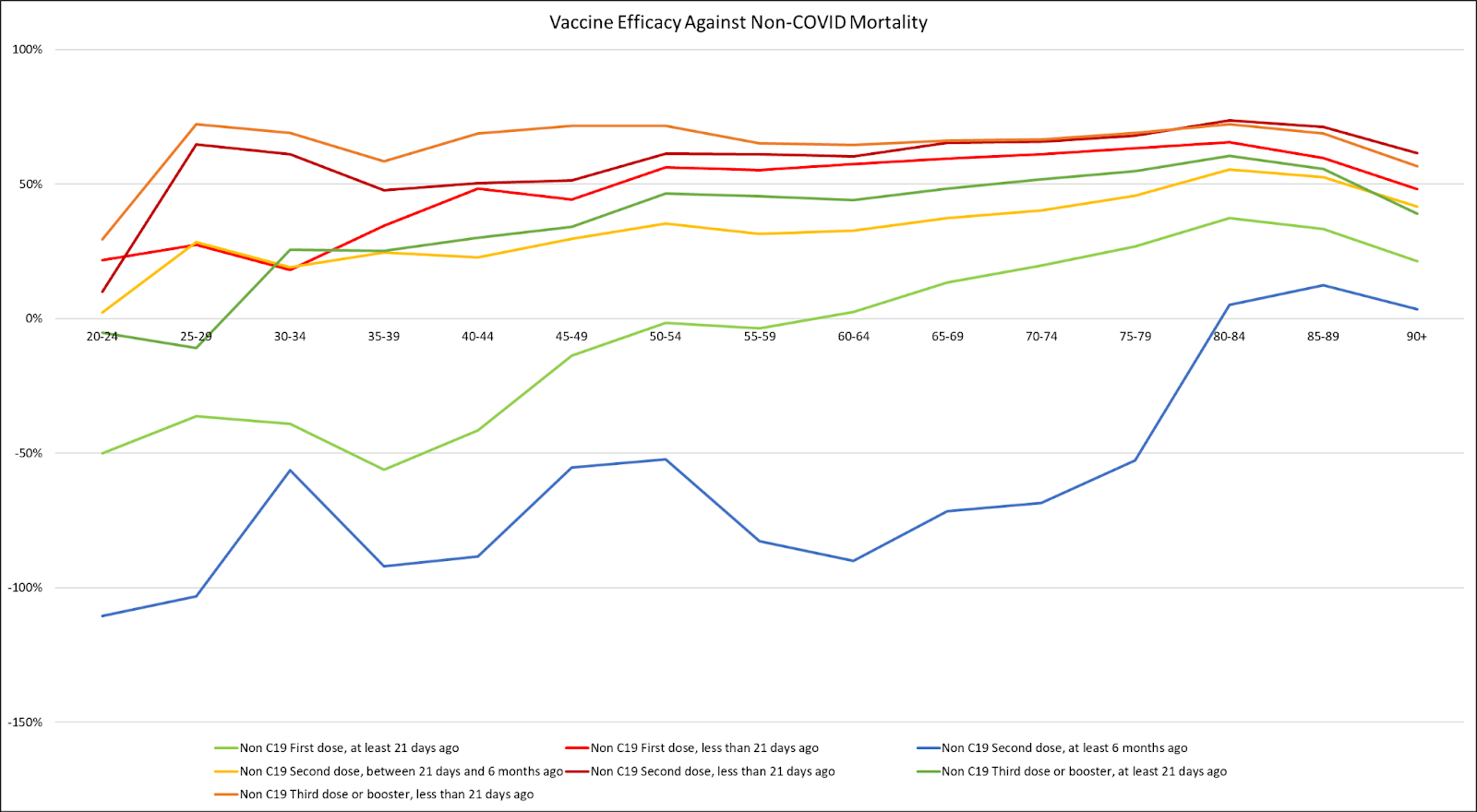
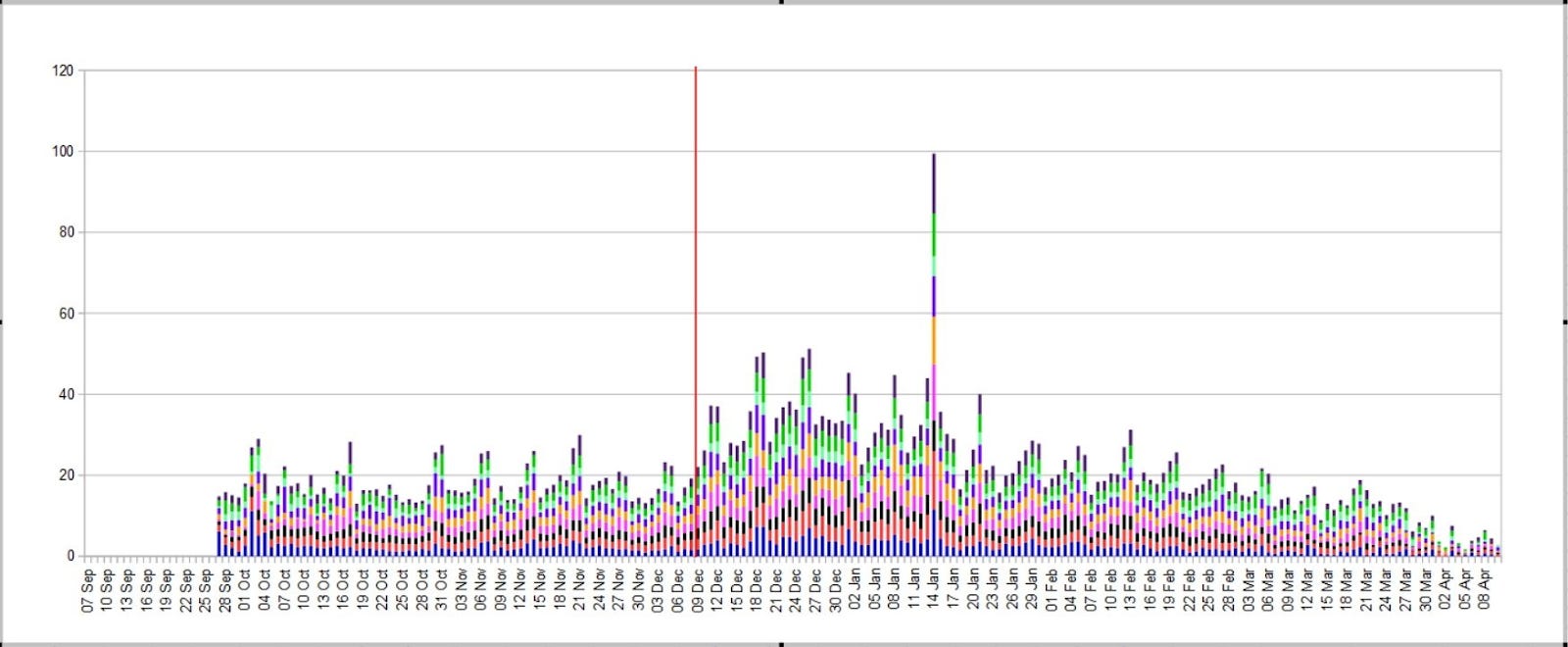
The top three data series (red/organge) are VE rates (against non-COVID death) during the first 21 days after first, second, and third doses.
The three middle data series (yellow/green) are VE rates (against non-COVID death) from 21 days up to 6 months (for the second dose).
The bottom data series (blue) is the mostly negative VE rate (against non-COVID death) for those who had their second dose at least 6 months ago.
Remember, these results should even take into account that 0.8% of those injected suffer serious adverse events (including death), which probably doesn't improve anyone's health.
Wouldn't most deaths after vaccination happen soon after injection, making this immortality effect even harder to achieve?
You ask a reasonable question, mysterious voice. Yes, VAERS data shows a substantial temporal association between post-vaccination mortality, meaning that most reported post-vaccination deaths happen quickly.
Given that there is no good reason for experimental COVID-19 quasi-vaccines to have [positive] effects on non-COVID mortality, and the waning pattern is similar to that which we see for COVID-19 efficacy computations, we should consider it likely that all VE calculations are compromised [by some sort of statistical sieve, including data tampering like pushing data into the wrong buckets].
Do we have [other] evidence of post-vaccination deaths being shoved into the unvaccinated bucket?
Yes. Yes, we do. Follow me…
Evidence of a Categorization Sieve
Many of us have suspected data shenanigans based on bucketing. But after reviewing the ONS data, I have a plausible explanation for how this could be taking place, aside from or in addition to something like Norman Fenton's "delay or mortality reporting" sieve simulation (which he notes, and we agree, is one possible explanation, but that a categorization sieve should also be examined).
First, let us consider the proportion of all deaths due to COVID-19.
Note that there were just over 77,000 (reported) COVID-19 deaths in the UK in 2020. Setting aside the last few days of the year, this gives us a solid sense of the proportion of all the deaths that are specifically due to COVID-19 among a non-vaccinated population. This appears to be around 12% of all UK deaths in 2020, which is almost identical to what I compute for the U.S. in 2020 (371k COVID deaths about 3.1M deaths).
{kind=link}
Two thoughts:
The short period at the end of 2020 includes some person-days in the vaccinated "bucket" (per data category), so there should be a very small correction factor when we use the overall data to compute the proportion of COVID-19 deaths among the unvaccinated population. As we will see, the overall 2021 numbers look very much the same as the 2020 numbers, so I'm not terribly worried about it.
While COVID-19 supposedly got going killing people in the Spring of 2020, that 12% might be a slight undercount. The first wave was likely just a delay of the Winter wave that would have straddled years, so I think this effect is small, like maybe ~13% of the deaths should be COVID-19 (as they're counted, which may or may not be appropriate, but that's another story) among an unvaccinated population. Yes, I'm (obviously) open to sensitivity analysis on that rough 13% number, but it's a very reasonable starting point.
So, what do we see among mortality numbers in the UK during 2021?

Here is a picture of the three bottom lines, graphed with the youngest cohort excluded (too little data, too noisy for the kiddos):
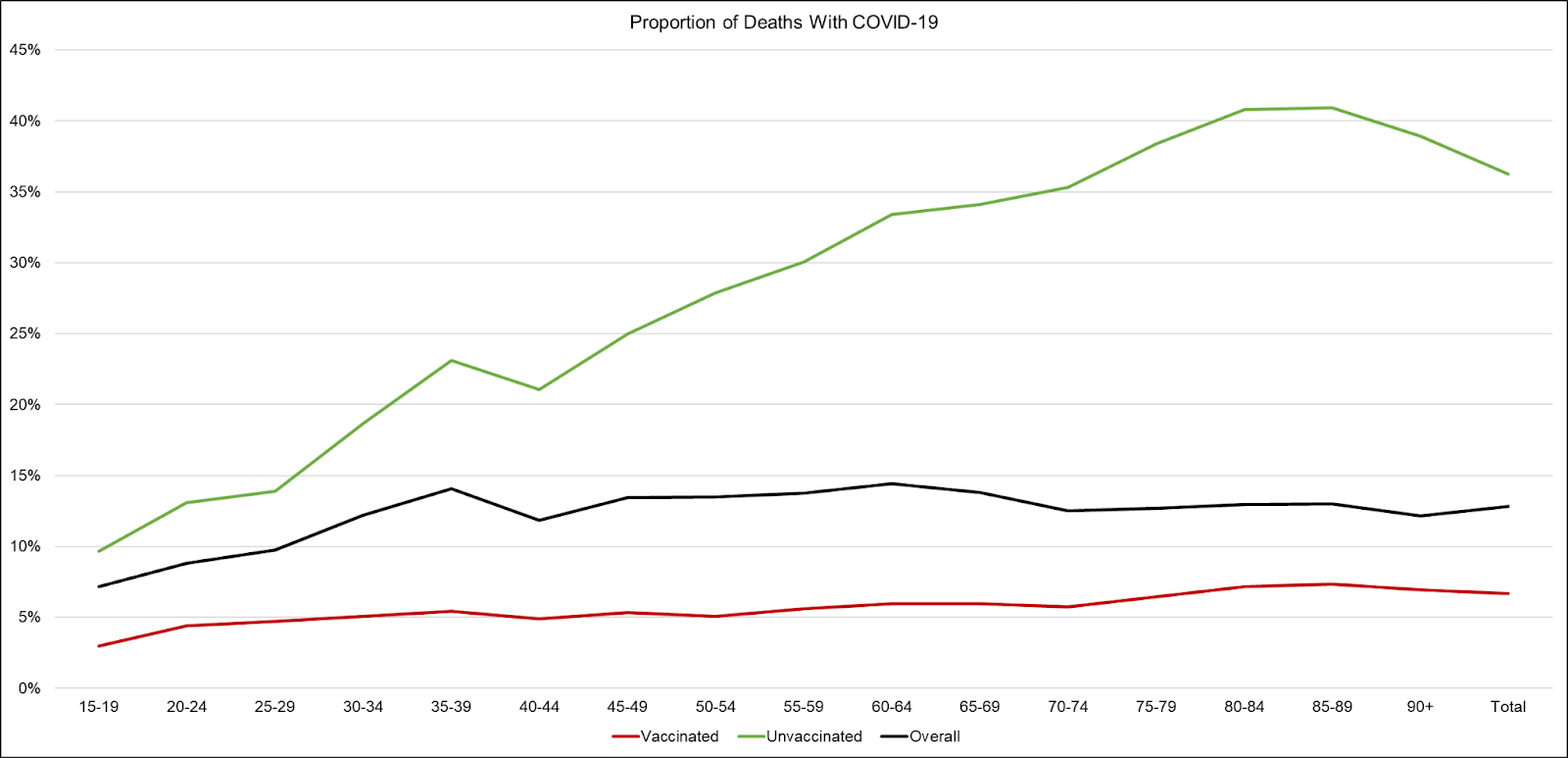
We see an overall COVID-19 mortality proportion of 13%. This COVID-19 mortality proportion is extremely consistent for those 30 years old and above.
That proportion is supposedly 36% for the unvaccinated! This proportion rises dramatically from the young to the elderly.
Whoa! Are we supposed to believe that the unvaccinated COVID-19 proportion jumped from ~13% to a whopping 36% between 2020 and 2021?! And that meanwhile, the overall COVID-19 mortality proportion just so happened to remain at 13%?!
Phrases like "shenanigans" and "horse shit" come to mind. But maybe there is a bias that explains this? But if there is a bias that fully explains this, then it tells us that the unvaccinated are specifically among the highest risk across all age groups. Is that possible?
If that's possible, then the mass vaccination campaign was a demonstrable failure because all the wrong people got vaccinated.
The implication that the unvaccinated are a much higher risk group needs to be taken into account and would dramatically slash all VE calculations to negligible amounts.
COVID-19 deaths in the UK during
2020: 77,071
2021: 75,163
Consider that we should expect fewer deaths in Year 2 after natural immunity begins to protect more and more of the population. At best, this feeds my argument that VE is and has always been an illusion.
Next, recall that my first vaccine mortality analysis was kicked off when I saw case fatality rates jumped in the UK starting the day of vaccine rollout:
Now, I have a new hypothesis of how the data is being manipulated. Call this the "Discrete Person-Day Hypothesis" or DPDH.
Consider a circumstantially healthy person (useless eater or otherwise, but not showing COVID-19 symptoms) who goes to get a vaccination at a pharmacy or hospital or Auschwitz or wherever that takes place. At the start of the day, this person is "unvaccinated" and in the "unvaccinated" bucket.
Then somebody pokes them with a needle containing a still redacted list of ingredients, known as a COVID-19 vaccine. Upon getting jabbed, that person dies.

Now, this person might be posthumously tested for COVID and found to be positive (whether real positive or false positive, they were not showing COVID symptoms) and called a "COVID death". They might also be described as having COVID symptoms between getting jabbed and dying, and thus a "COVID death". Or, they're a non-COVID death (more often than not?).
But here's the important part: whether or not they're counted as a COVID death, they were unvaccinated at the start of the day, and that person-day might still be counted as an "unvaccinated day" because the system may not be set up to record anything more than a day (not time) of vaccination.
By the DPDH, a person could get vaccinated and die on the same day, but that day would be recorded in the "unvaccinated" buckets with respect to the system.
Think about what all this would explain:
This would explain the increased case fatality rates we see not only in the UK above, but all over Europe during vaccine rollout.
It would explain the baffling immortality effect.
It would explain why there are demographic specific VEs in the data that do not show up as systemic effects.
It would explain why the unvaccinated appear to die more often around each vaccine rollout.

Of course, the authorities would know full well if this is going on at the database level, with these miscategorizations, so they would (1) never release raw data, and (2) hold back data (as the CDC has admitted to doing) that might shed light on the nature of the statistical sieve.
So, tell me what you think of the DPDH. What are the chances that this is what's going on with national data?
Addendum 1: I meant to talk about this, but came up with the DPDH in the middle of writing the article and focused on that. But there is a Notes tab in the ONS database that mentions 2,044 people who died shortly after vaccination who were not included in the National Immunisation Management Systems (NIMS) used by the ONS. Hello! This alone throws into question all the calculations, except that we do not know where to bucket this data.
Addendum 2: As I said, I haven’t looked at the ONS data as much as some have, but there is a paper explaining what appear to be data shenanigans further (Neil et al, 2021) which I have now partially read at this moment. I’d seen it previously, but my focus on DMED and other data kept me from soaking it up.
Addendum 3: An Israeli professor was apparently watching this "pseudo VE" back in November and worked up a solid Twitter thread on the topic.



I suspect I will have multiple addendums since this hypothesis is being bandied about by a few people, and some may have observations that jibe with it.
Just woke up so still groggy, but aren't they still counted as unvaxxed until 2 weeks after their (latest) jab?
Of course there are shenanigans going on. Heck, they've never even proven that "regular" (pre-Covid) vaccines are effective in the long term. The whole thing is a giant myth birthed by the Great White Polio Panic of the 1940s and 50s (when they used to literally think black people were immune) combined with the WHO finally getting a win in the 70s with their smallpox program. When the WHO was founded, the two big issues were cholera and malaria, neither of which has ever shown any improvement whatsoever.