


Is This What a Successful Vaccination Campaign Looks Like?
The Vaccine Wars Part LIV

"A foolish consistency is the hobgoblin of little minds, adored by the little statesmen and philosophers and divines." -Ralph Waldo Emerson
Prior articles about the Wealth Theory of Vaccine Efficacy and other Vaccine topics can be found here.
Last week, I published a re-analysis of the Society of Actuaries report that made the rounds.

A response by COVID-19 Data Science blogger Jeffrey Morris butchered my entire article—either out of laziness or bias or malice (I think the former two, most likely). He incorrectly stated that I,
Used data from the (months) older report, even though it's clear in the article that I downloaded the most recent CDC data that was newer than the latest report.
Ascribed to me a strawman view of causality that is askew from anything in the article or anything I've ever stated and argue against often.
Characterizes my critique of him (as selective in his applicatication of principles and statistics) as "ad hominem", and while I do poke fun at him often (because I think somebody at his level of authority stumbling so often without self-effacement should be the subject of a bit of comedy…I consider it kind considering what global mortality data looks like right about now).
Jeffrey is a great example of somebody working in (support of) applied science who doesn't recognize his bias from indoctrination. Is it ad hominem to point this out? This is from an email exchange on July 23, 2021:
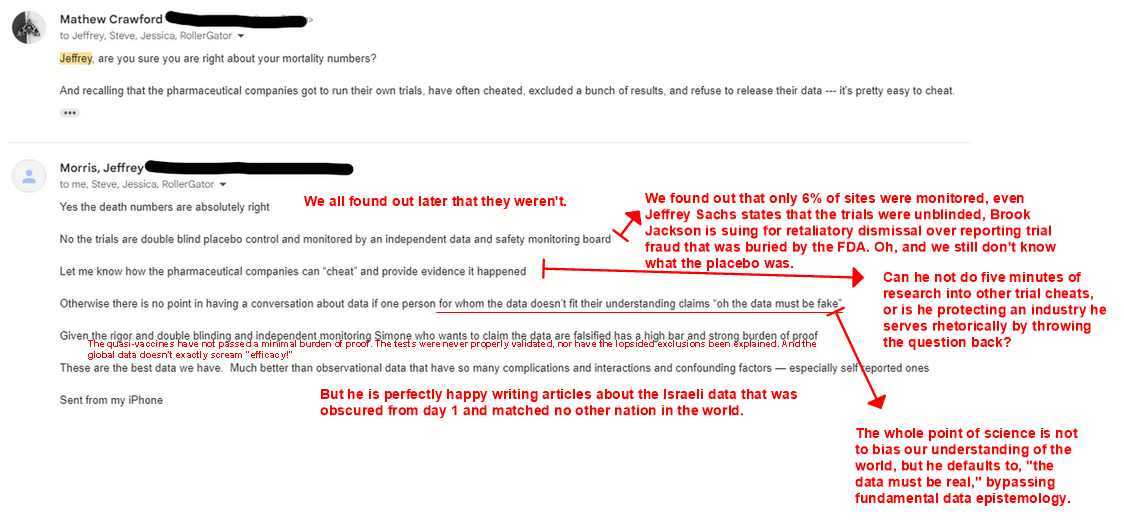
What he didn't say in his article is, "My beliefs a year ago were founded in these things that are now pretty hard to defend in retrospect," or, "Maybe I should have mentioned to my readers (since I'm an expert) that these were the first vaccine trials in modern times not to validate lack of confounding by the disease testing process." He seems to recognize the confounders everywhere but at the source of his default bias. Why wouldn't he? These are good people.
Further Analysis of the CDC Data - Is This What Efficacy Looks Like?
Data sources are in my article as linked above. Same data set from around a week ago.
Let's start with working age adults, age 25-44. Focus on each region, one at a time. Do you see deaths going down prior to the Spring of 2022?

I highlight 2017 and 2019 because either could be the initial release/escape of SARS-CoV-2 or some other SARS-CoV that we're not told inhabits the quasi-species swarm cloud.
Recall that these are excess deaths, so absent other factors, we should see mean reversion—particularly during down seasons for SARS-CoV-2 infection. In fact, during down-seasons for viral infection, we should see negative numbers counter-balancing the positive numbers even assuming a null saline solution with zero efficacy. What gives?
Remember that COVID-19 has a mortality curve that is startlingly similar to the general mortality curve—or at least it did through February 2021 (Shim, 2021).
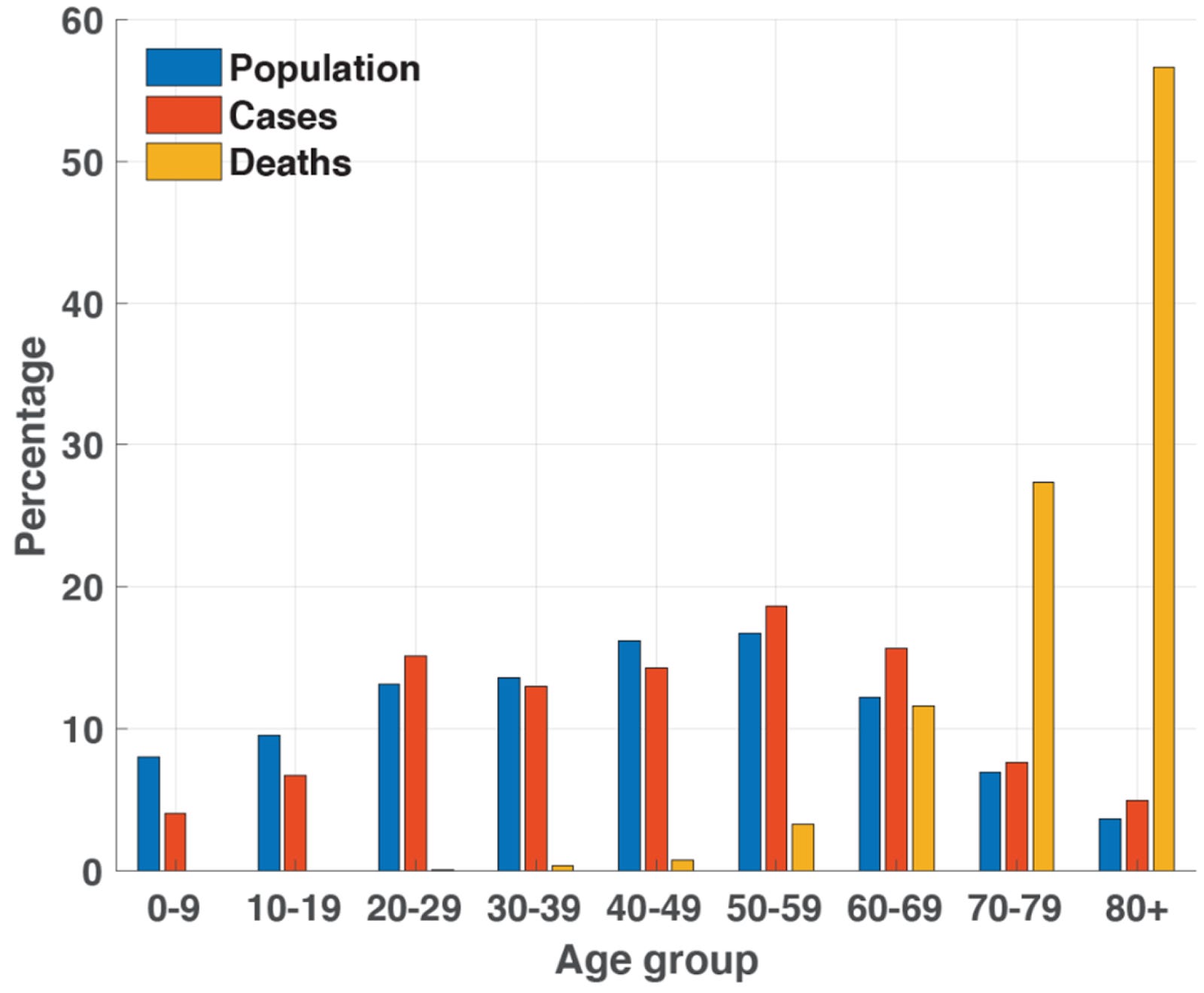
Back then, essentially no healthy children died (Makary, 2020), and the number of/with COVID-19 deaths of healthy people in their 20s, 30s, and 40s who died was so small that they might have represented only those people who suffered from specific and nearly invisible genetic disorders that resulted in autoimmune conditions in the event of SARS-CoV-2 infection. For instance, auto-interferon antibodies have been found in up to 20% of all COVID-19 deaths (Bastard et al, 2021). And that even assumes that some of those deaths weren't false positives or died (merely) with COVID-19.
If the vaccines are safe and effective, those who had died were a substantial subset of the most vulnerable, why on Earth would young people start dying in larger numbers as more and more of them got vaccinated?
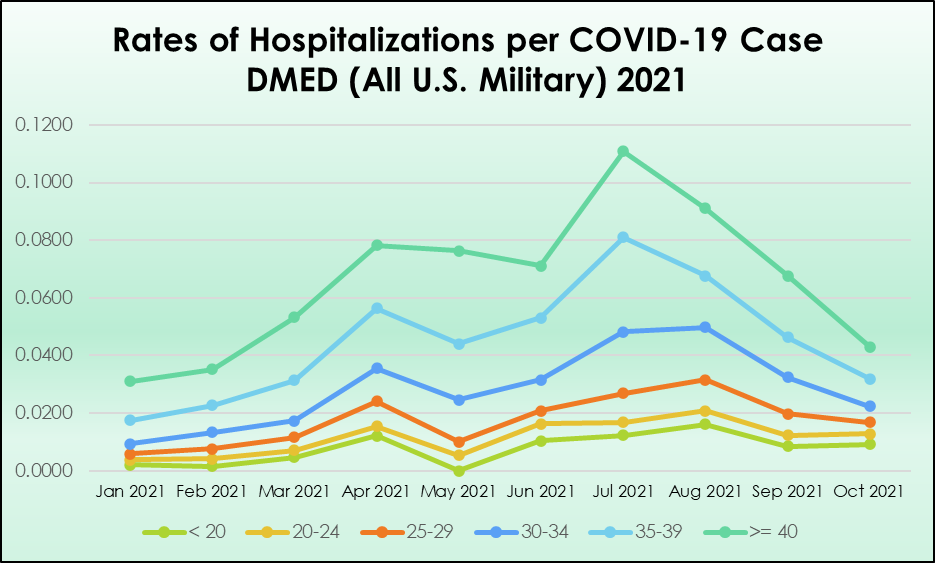
Recall that this is a cohort similar to that of the U.S. military (which is slightly younger than the broader population above). What we saw in the DMED data was the severity of COVID-19 worsening each time vaccine administration ramped up (early in the year, then heading toward mandates in August). Hospitalizations per case quadrupled. That's in addition to the fact that COVID-19 cases went up 70% in the military (2021 vs. 2020), and there were nearly as many cases in January 2022 as in all of 2020.
Tell me what you see, Jeffrey? Or should we continue to talk context? Or more context?
Are you sure you can defend with a straight face that there's no evidence that points to shenanigans?
Now let's take a look at the older half of the working age population.
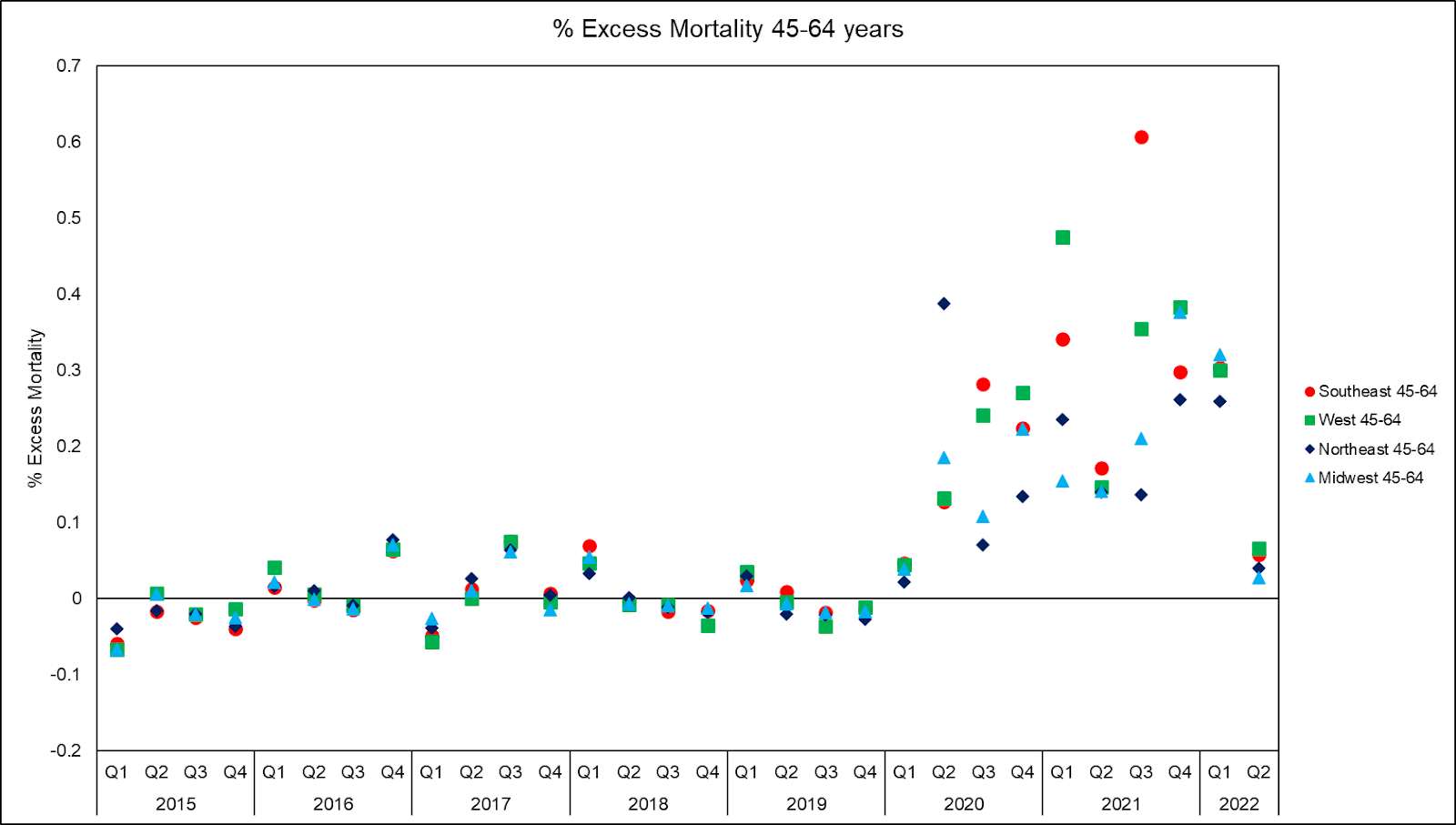
Again, excess deaths continue to plow upward despite vaccination until after Omicron cleared the board. Next up, the maybe-recently-retired.
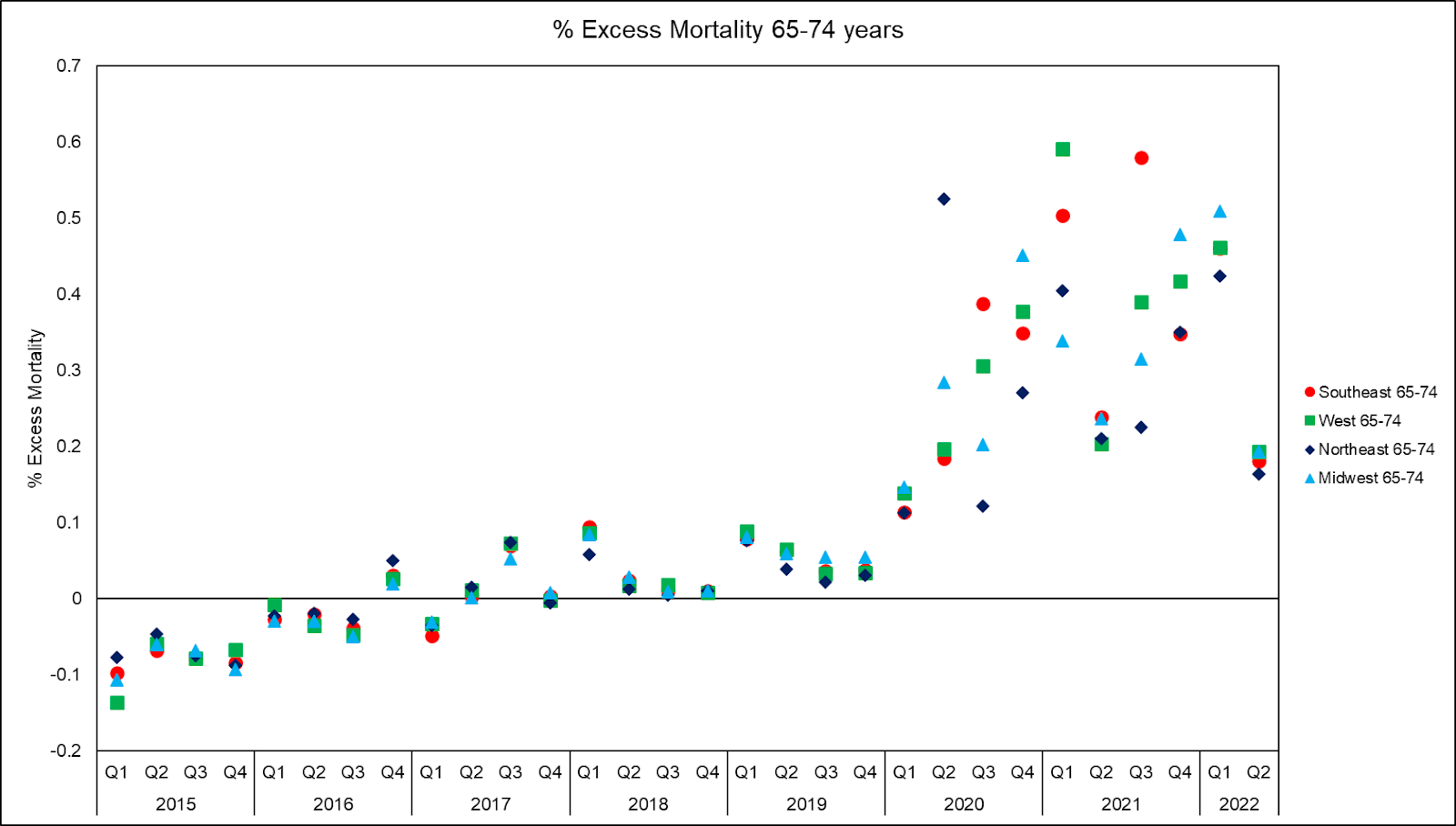
When we're looking at 10-year age bands, there can't be too much of a Simpson's paradox.
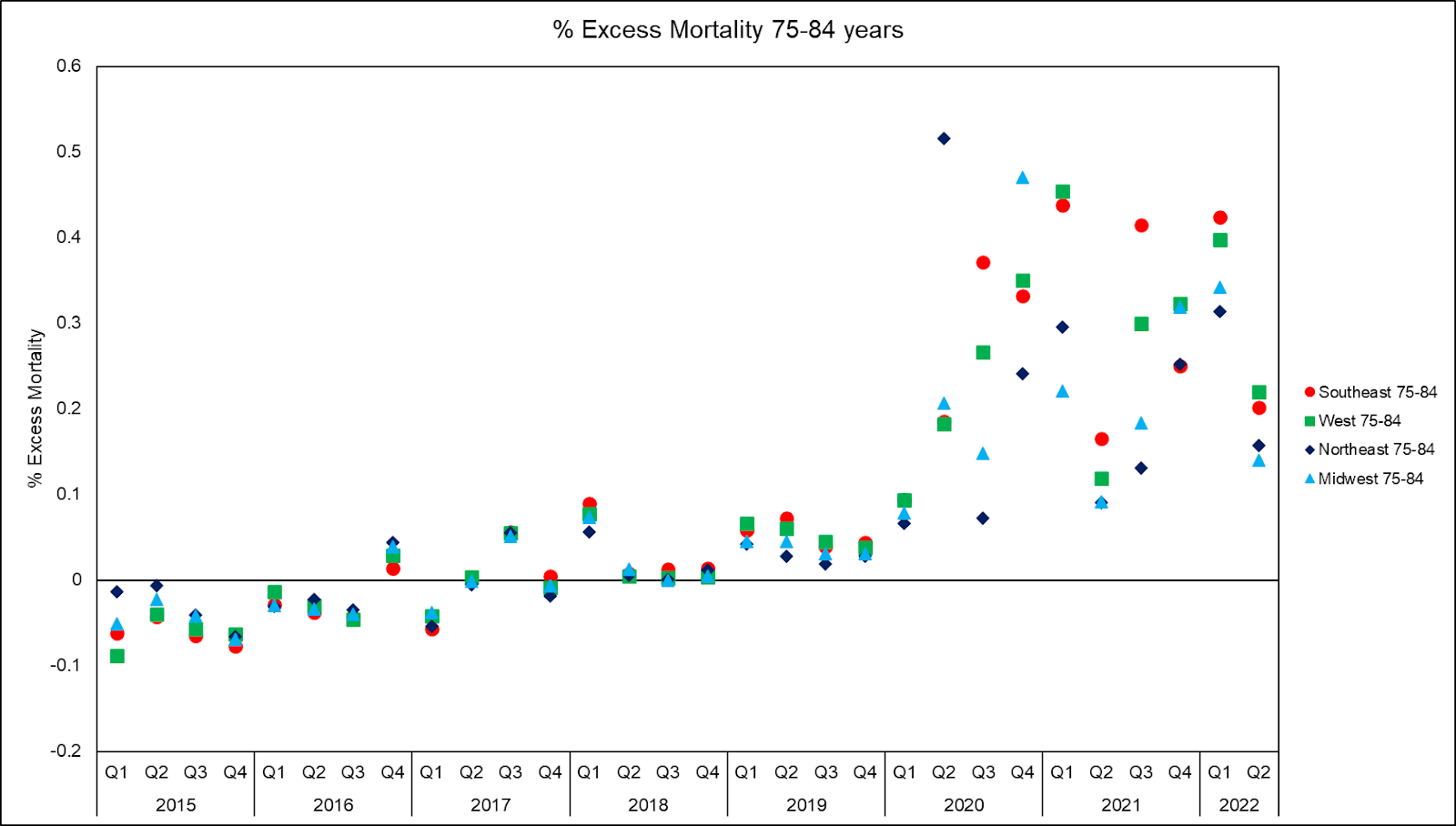
It's only when we get to the oldest Americans that we see…something that might…let's just look:
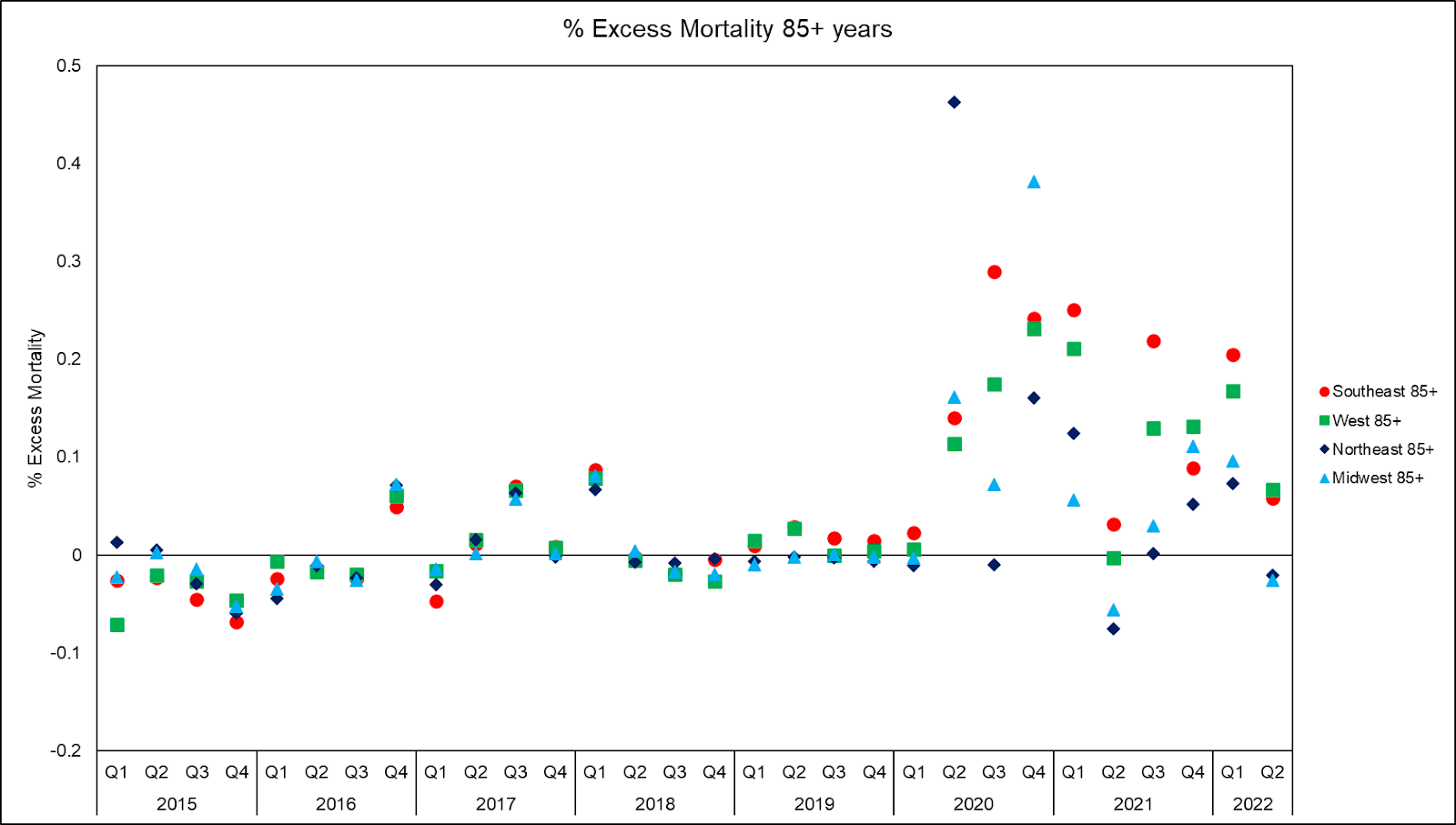
What we have to note here is that somehow, for whatever reason, people in nursing homes just sort of stopped dying of COVID-19.
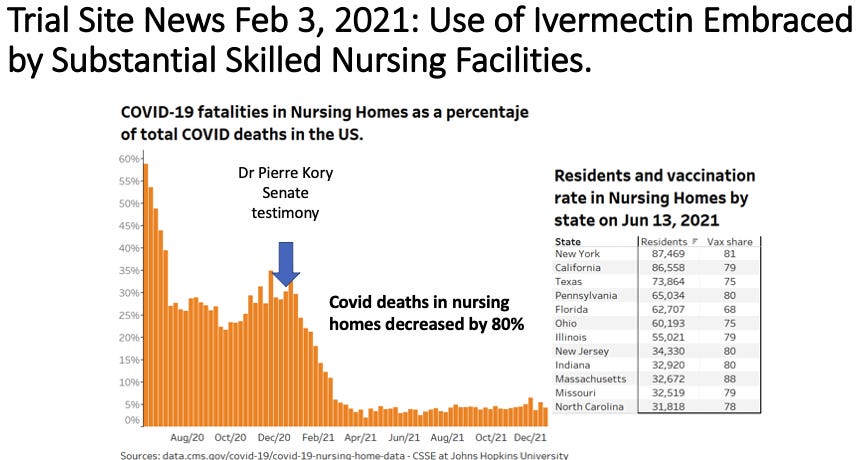
I'm not saying that's because of ivermectin or even hydroxychloroquine, which likely increased in usage more among those most capable of standing up on their own to turn off the TV and go do their own research than somebody in a nursing home. I think antivirals probably helped most the elderly outside of nursing homes. What I think is that it's awfully unnatural for this particular group to plummet as a proportion of those succumbing to a particular illness. If this were due to vaccine efficacy, we would have seen similar reductions in mortality in other cohorts (and counties or states with extremely high vaccination rates), and that would have brought back up the proportion of nursing home patients dying of COVID-19.
If you're wondering if the nursing home deaths dropped due to "burning through those most at risk" (much like excess mortality mean-reverts), understand that the graph above is a proportional graph, meaning that it should remain relatively stable if deaths in all cohorts decline, all things remaining equal. But what we saw instead of nursing home patients tanking as a proportion of COVID-19 deaths, without any particularly good explanation.
There is some point at which you have to stop and wonder whether what took place in the nursing homes, and among the mentally ill in 2020, was iatrogenocide to set the stage of the quasi-vaccination campaign. At least, recognize that there is a certain level of data consistency that holds better than most of the competing narratives.
Your ridicule of the fool was too kind and generous.
I personally know of a nursing facility owner who was following my work, which led to Kory's/FLCCC's work which led to them adopting IVM use early on. They reported vastly lower case and death counts as compared to even the gen pop. Crazy, right?
As explained, there's an economic angle. The hospitals were paid to put people on vents & Remdesivir, and even though that killed people, that was their motivation.
For nursing homes, filled beds/rooms is the economic motivation. So they were motivated to find solutions.
Time for us as a culture to examine the power of money over our lives, is the message I believe.