
Remain Calm and Keep Learning
The Education Wars Part XIII

Other Education articles can be found here.
Most of the time it is best to remain calm, and keep learning. We should certainly at times express our genuine outrage. We should also keep our outrage on a leash that doesn't interfere with the process of self-correction. No one of us has been right about everything going on during the pandemic, but it's important to remain open and be able to discuss matters with people who are ready to discuss.
Last night I published an article explaining what I feel like is a pretty logically tight argument that unless there is documentation that I haven't seen, and so far nobody I know including Robert Malone has stumbled on, that the tests used to assess disease (or "disease") in the vaccine trials were validated for similar sensitivity and specificity between the vaccinate and the unvaccinated (that vaccines do not confound the test), that the trials were simply and plainly invalid. I leave the door open to being wrong, but if I am, the exploration will open new doors and opportunities to learn. One way or another, I feel that this is one of my most important articles.
An interesting thing happened in the discussion threads. It started here:
Those who know me or began following me at any point in time are aware that I am a critic of the way polymerase chain reaction (PCR) tests have been used during the pandemic. In this article I'm going to explain a piece or two about the manipulations that I suspect most people haven't yet heard. Prior to the pandemic, I knew a basic bit about them, but quickly learned more through my wife who is a biochemist and frequently designs PCR assays. The sorts of assays she designs are a bit less controversial than viral diagnostic testing "in the wild". As a tool, PCR is easier to handle in laboratory settings without much risk for contamination by "off target amplicons" (genetic interlopers that contaminate a sample, then get swept up by the primer and replication process, eventually cycling up to the point of a false signal. That can still happen in a lab, and there is literature on false positive rates with respect to cycle counts, but for the moment I'm going to keep the discussion focused on the issue of diagnostic testing during a pandemic.
Controversial Biochemist Kary Mullis
During the chaos of the pandemic, those doing their own research discovered the story of Kary Mullis, inventor of the PCR technique.
His whole ("whole basic") story, which I've gradually read about, is instructive on many levels. It's interesting to hear him talk about looking for applications of his procedure in order not to have to lay off his employees. That immediately tugs at my heart strings. I often go on walks just in order to meditate on how to employ people synergistically with my business and goals. But Mullis found that the sharks of industry were even more creative (or "creative") about finding ways to use PCR, and to a point he believed invalid.

This is a great example of the linguistic confusion that has been sowed by the biomedical community with the help of the World Health Organization (WHO). Under the classical (sensical) model, you
Test for infection.
Diagnose disease (defined by symptoms, not infection).
I'm going to stop here and say this: there is a way to deploy PCR testing for viral or other genomic surveillance that can provide great big picture data. So long as you're aware of the potential confounders in order to make appropriate use of the data…you can make appropriate use of the data. And it is easier to make big picture statistical arguments from data that is somewhat dirty on an individual granular level than it is to make diagnostic observations on any single individual "in the wild" outside of a laboratory.
Would Kary Mullis agree with me?
Kary: "I don't think you can misuse PCR…"
I love it! My own dictum with respect to data is, "All data is useful." The art is in understanding the data as completely as possible. This is part of the reason my work as an applied statistician is often more wordy than equation-filled. The explorations of the logic by data are 99.9% of the process. Kary's point is that the information that results from PCR gets misunderstood and misused (his words). That he set the stage with the above quote first shows you how much he has thought through the discussion in order to explain it well.
But I think it's safe to say that Mullis agrees with me here. We can detect infection within bounds that we can calculate. We can talk about those bounds.
False Positive Rates
Those who have not worked with data a great deal may not know this, but false positive rates are not static, invariant numbers. They change over time—and by a lot.
Note, this is the extension of the first thread about whether those who are vaccinated and those who are unvaccinated were ever tested using different cycle count thresholds. That certainly did not happen during the trials (by any documentation I have seen, including links she provided). What did happen was that after Biden came into office, the cycle count threshold for virus detected in the vaccinated was lowered (to 28 IIRC) for the purpose of choosing those sample sent for full genetic sequencing. This is distinct from the use of PCR as a broad diagnostic tool, though I have seen the claim made and propagated that testing surveillance was distinguished in this way. That strikes me as disinformation or misinformation, and our community that is resisting authoritarianism should be careful about how we communicate facts, and sometimes take some time to give more complete explanations in order to limit confusion. Further, people of good faith who find that they were confused should then learn to dig deeper and have discussions with more people to seek greater understanding before pushing what could be mis/dis-information.
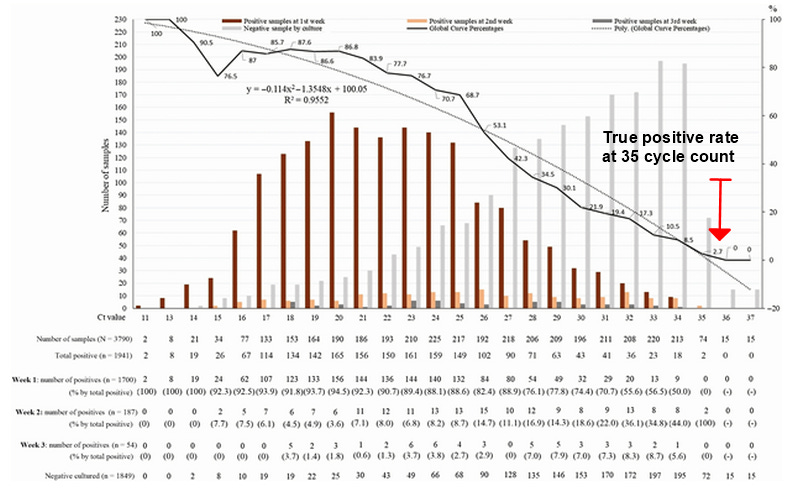
The 97% number comes from a paper (Jaafar et al, 2021) at the high PCR cycle count of 35, meaning the process of replicating each genetic sequence swept into the PCR process is doubled 35 times. An off target amplicon might be swept up at any point in the process, so maybe it gets double 19 times at which point one individual sequence of nucleotides results in a total of 524,288 strands, which is quite measurable. But even the intended target amplicon gets ratcheted up to around 34 billion strands. So, some tiny amount of virus that a body is successfully fighting off, or even some artifact strand from a prior exposure
With respect to mass diagnostic testing, this is quite concerning. It means that testing parameters can be chosen to sculpt the appearance of a pandemic to suit some purpose. And I will make this clear: I have little doubt that such intentional manipulation has taken place! I personally believe that the SARS-CoV-2 virus was already circulating widely in 2019 (and likely before), but isn't a particularly big killer. I have seen signs of it in numerous data pools, and I have begun documenting some of that in the Plandemonium series and elsewhere.
The Evolution of False Positive Rates During a Contagious Outbreak
For a lesson on the computation of false positive rates, refer to my article from April of last year, which includes a video discussion.
Let us dispense with any discussion of the limited use of SIRS and other models that have varying levels of conformity to reality. We all know that the map is not the terrain. The purpose here is simply to examine what happens to false positivity rates during an epidemic, and the range of the false positive rates is the same for any epidemic that starts at 0 infections and peaks at the same levels as our graphs.
Example 1: For a population of 10M, using R = 2.5, and a test with sensitivity 99.2% and specificity 99.4%, the false positive rate drops from 100% to 0.6%, then back up to 100%.
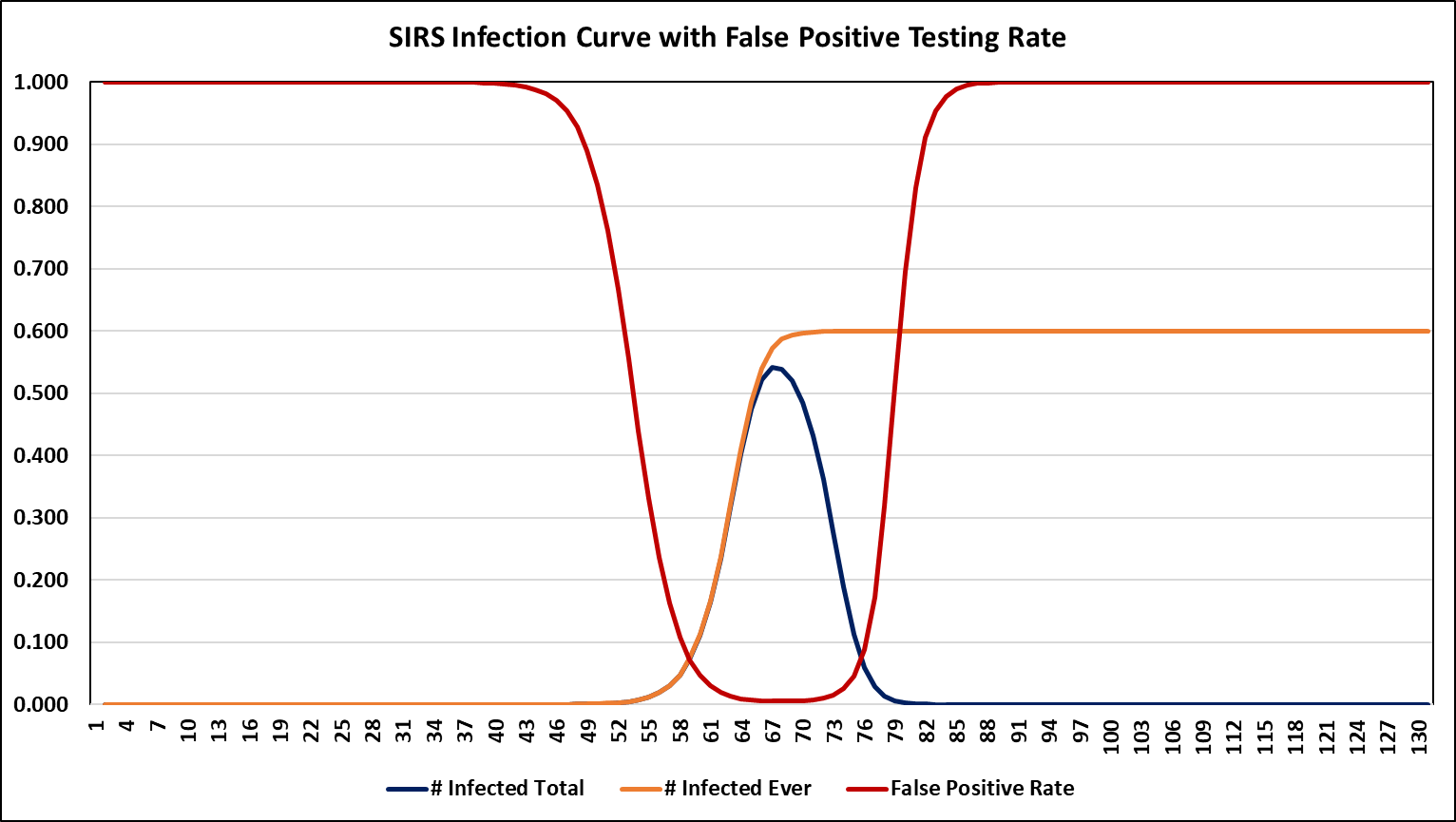
Example 2: For a population of 10M, using R = 1.82, and a test with sensitivity 97% and specificity 95%, the false positive rate drops from 100% to 7%, then back up to 100%.
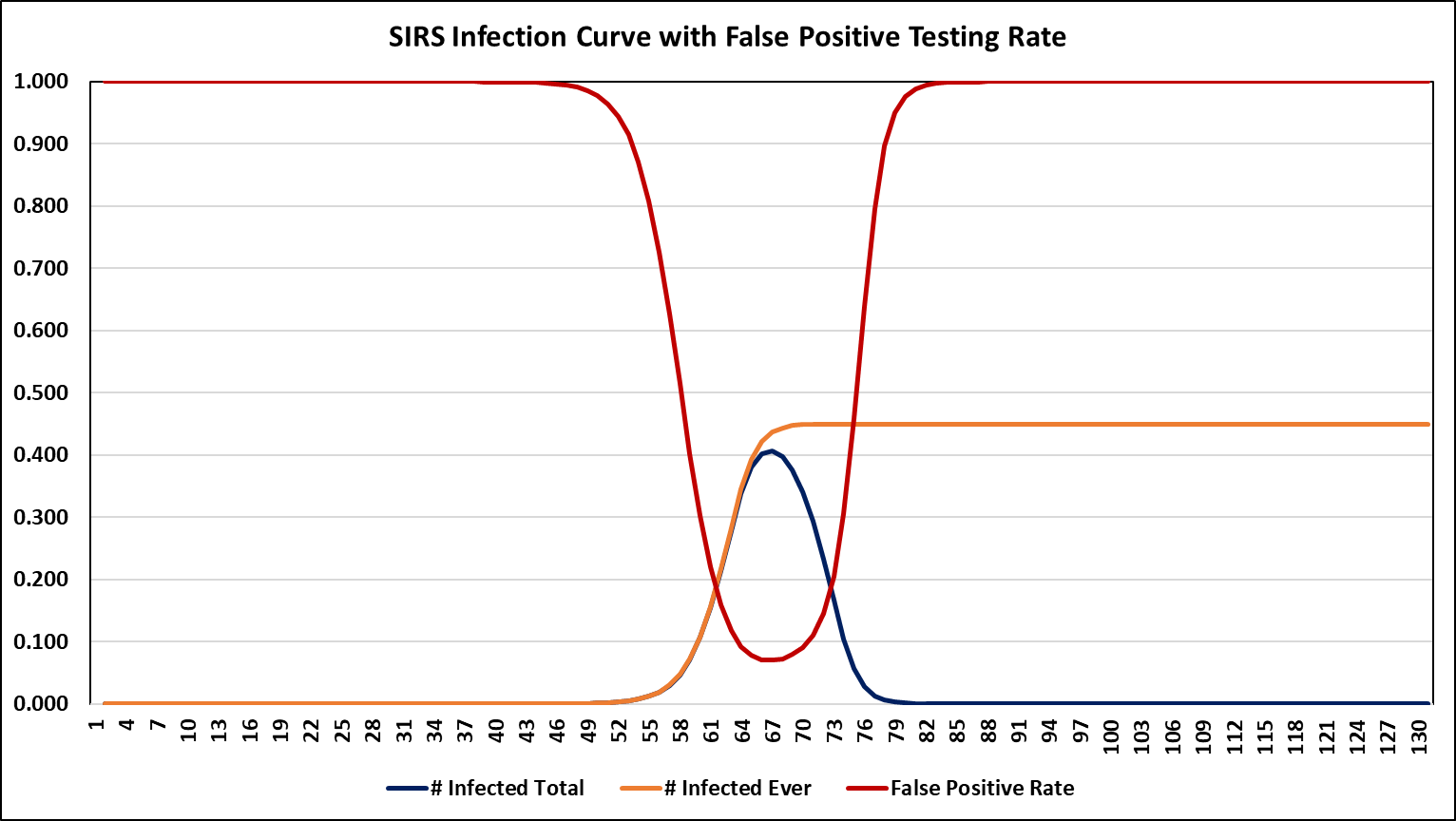
The point is clear: this is a whole lot of variance. And we do not even know something like the mean false positive rate without knowing how much testing was going on during each point in time!
Remain Calm and Keep Learning
Much of what I know about epidemiology I learned during the plandemonium. I also learned how little most epidemiologists know, and how terrifyingly poor and deranged their body of cookie cutter statistics is, but those are stories for another day. The several high quality epidemiologists must feel depressed watching thousands of degreed zombies added to their field each year.
But there, I've expressed my outrage. And better, I didn't aim it wildly at people I didn't know on the internet. But here is an interesting sample of Joy's (which is apparently a researcher of some kind) comments toward me.
It's…my feed. And if I'm part of the Pharma propagandist pool, everything is much, much worse than anyone has yet imagined.
But obviously, this is wrong (unless I'm shredding the Pharmafia en route to selling one gigantic lie on their behalf…so maybe don't listen to me when I suddenly start selling that new brand of untested nonsteroid pain killer made from opioids and cricket flour). And it may be good to meditate on the times we feel angry over people disagreeing with us. It may not actually be because they're on "the other side" or "part of the depopulation agenda". There may be opportunities to learn that are lost in the tunnel vision.
But at least we made this an educational exercise.
One last thing: Understand that when it comes to conflict with most people…and I mean most people…I prefer to take the honorable road.
Also…well…also…
The mere fact that you suggest people “keep calm” and “keep learning” is proof enough you aren’t part of the cabal, who’s motto is “shut up, and freak out over the issues we tell you to freak out over, when it’s politically expedient for us.” (Trust me, it sounds much better in Latin).
I found the article re: injections and negative tests in the presence of symptoms fascinating and an entire different way of looking at the past 20 months.
Two points. 1. After reading 1/2 of your article yesterday, I took the dog for a walk. While walking, something was tweaking at my memory. It finally came to me. I was doing some reading years ago on cancer drugs while working on an unrelated project. I can't pull a reference, but the gist of it was the standards for getting the chemo drugs to market were based on endpoints that were not related to longevity in some cases. E.g., a tumour reduction of 20% would result in approval of drug. A tumour reduction of 20% would not significantly impact endpoints of significance to the patient. That was an eye-opener. Similarly, if the c19 injections result in negative tests, but otherwise no significant degree of disease reduction, this is of little consequence to the injected, and could actually contribute to spread of the virus if the sick think they are not harbouring C19.
2. Aggressive tweeters are the worst. Especially when they've no idea of how you have been working hard to out the numbers and manipulation of data. However, after the way the data has been manipulated and hidden in cases, how can we know with certainty PCR cycles were not manipulated too? Anecdotally, we've heard nurses claim that the charts for people coming to ER were marked as UV at the top if the record of injection was not associated with that same health system. Nurses claimed when flipping through the file, often the opposite was true. Likewise, anecdotal reports have surfaced of treatment protocols being varied for un-injected vs injected. Anecdotal, I know, and that is not the way of data, but I would not put anything past those incentivized to push their injections and deaths for money. Similar to the climate "emergency" they will do whatever it takes to fool those who are too busy, lazy, trusting or frightened to look beyond the headlines.
Thanks for more "food for thought."