


Who Died During the Plandemonium? Exhibit A
Plandemonium, Part 2

"Sometimes, the aftermath is more devastating than the storm. That is the story of the 2008 financial crisis. It was disastrous at the time, but what has been worse is how long it has lingered." -Chrystia Freeland
Data sources can all be found at the bottom of this article. This is also a time to mention that this article will kick off a Monday evening (for now) weekly discussion at Clubhouse.
For the purpose of this article, all correlations are with respect to COVID-19 deaths.
Graphs with white backgrounds are always correlations between values measured on a particular day (or short trends like 7-day averages).
Graphs with the black backgrounds are of correlations that involve one or more cumulative measurements.
I will try to make that clear as I go. No promises.
Here is an example of a chart we will examine. It shows weakly negative correlations between (cumulative) vaccine uptake among counties and 7-day trends of COVID-19 mortality. What do we see?
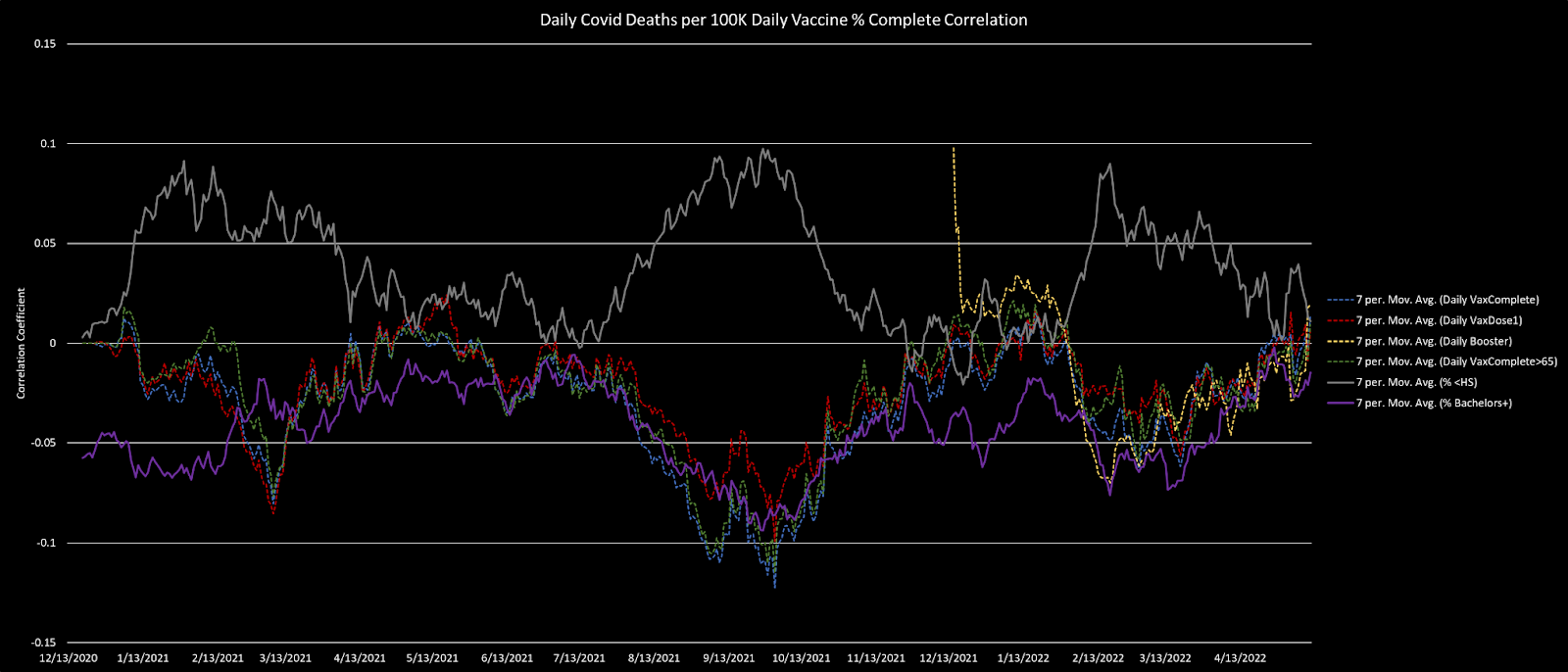
Spoiler alert:
There is very little difference in these correlations between county rates of those who have taken at least 1 dose of an mRNA vaccine, those with a full vaccine series (whether 2 mRNA doses or 1 of Jannsen's vaccine), those with boosters, and the proportion of the elderly (>65) who are vaccinated.
These correlations are almost perfectly tracked by education status. This raises questions of causation of the mild advantage seen among counties where vaccination took place more widely.
For around a year, I have suspected that there is literally no benefit (with substantial evidence of harm) in terms of COVID-19 mortality or disease conferred by the experimental quasi-vaccines. I'll call this the Crawford Zero Vaccine Efficacy Hypothesis (CZVE Hypothesis). Here is a basic summary of the evidence:
International data shows COVID-19 cases and death increasing with experimental vaccine rollouts. The correlations that we would expect to be negative if there were any efficacy at all are consistently positive.
Experimental vaccine rollouts are associated with greater levels of COVID-19 mortality across all of Europe, suggesting survivorship bias contaminates a lot of data.
State level correlations data shows almost no consistency that we would expect from any substantial vaccine efficacy (VE).
Hospitalization rates have been gamed, but data is starting to reveal a lack of efficacy (here).
There is a tremendous pile of evidence that fraud occurred at multiple levels during vaccine trials, some of which very directly supports the CZVE hypothesis.
More Questions Than Answers
"It is better to know some of the questions than all of the answers." -James Thurber
That's where we are with a lot of the plandemonium. Do not expect some correlation data sets to illuminate everything for everyone. However, I do think the selected charts will help illuminate aspects of the Bigger Picture for some or many people, or at least to guide us along marginally better lines of inquiry.
The Partisan Question
"Judge a man by his questions rather than by his answers." -Voltaire
A few weeks ago I wanted to entirely dispense with the Partisan Question:

Having had longer to think about correlates to partisanship such as the way Republican/Democratic incomes diverged following the mortgage bond crisis, I am re-evaluating my position somewhat. After all, I have written about the ways in which certain aspects of pandemic propaganda played toward partisans:
What if there is something like the targeting of classes with better or lesser forms of care, and those classes notably break down along partisan lines?
The Elderly (and a Nuance)
The vast majority of the people who have died from COVID-19 are at an age that is 90% or more of the way to the life expectancy in their respective nations. Obviously, I only know that COVID harms the elderly much more thanks to the immense genius of the brain-o-rubric that is Bill Gates, through which all public health knowledge flows.

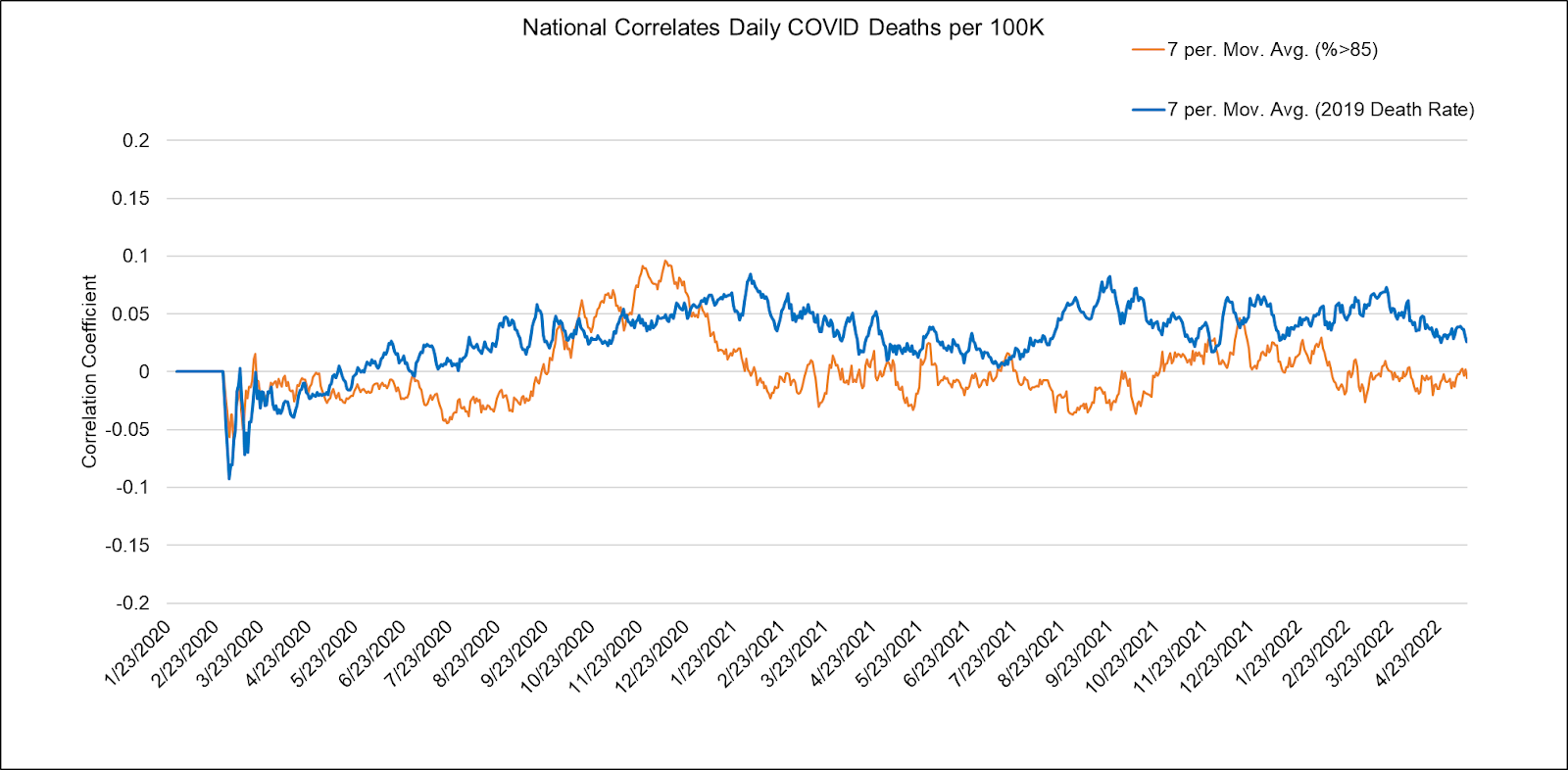
I do, however, have a maybe-original thought on the topic of mortality, which is that the spike protein found in the virus(es) and vaccines compresses life expectancy for those who already have problems. The healthy resist and repair the damage more readily [outside of hidden genetic abnormalities]. For younger people, mortality may be something like a disaster lottery, but it is interesting to see that the correlation between recent county death rates (2019) and COVID-19 death rates is one of the more consistent during the plandemonium. In other words, more people die of COVID-19…wherever more people die (are nearer to death).
Is There a Race Thingey?
"Darkness cannot drive out darkness; only light can do that. Hate cannot drive out hate; only love can do that." -Martin Luther King, Jr.
Yes, there appears to be a bit of a "race thingey" during the pandemic. And by that I mean that it appears that race matters [in some way]. But exactly how race matters is not simple to tease out (from this analysis alone). It may be best to take some ideas from these county level correlations, and then do deeper investigative work with more granular data sets.
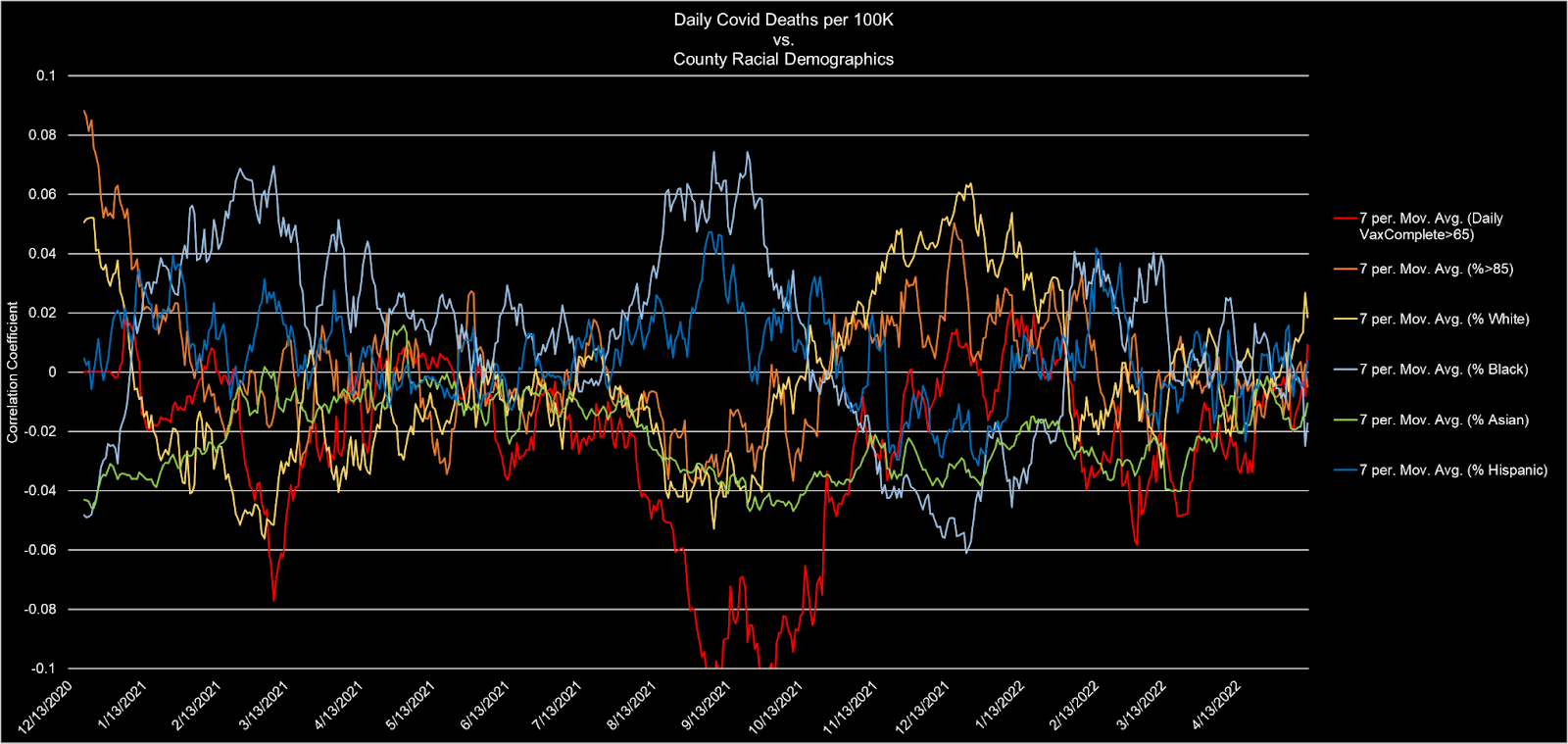
Several things about this chart disturb me:
The correlations between proportions of extreme elderly (>85) and COVID-19 deaths (orange) are stunningly weak!
There are positive correlations between COVID-19 deaths and minority (black/hispanic; light/dark blue) county populations that are largely between season. Why wouldn't these correlations be fairly consistent?! Are minorities targeted at some hospitals when infections are low as a way to justify pandemic fear mongering during times when essentially nobody is really dying of COVID as opposed to "with" COVID (or "with" a possibly false positive)?
The only time there is a significant [negative] correlation between vaccination rates for the elderly (>65) and COVID deaths (red) is when there is positive correlation with minorities. It appears that there is an excess of off-season COVID deaths among elderly minorities.
Note that while studies (e.g. Shimizu et al, 2021) show lower risk for COVID-19 in Asia, that Asian Americans suffer only marginally lower case and mortality rates. Further, there is every reason to believe that such marginal effects are primarily due to education and income levels (enjoyed to varying degrees by nearly all Asian American groups), as we will discuss.
Education and Income
Education leads to greater wealth. Wealth leads to greater health. Assign causation however you like, but do not forget the relationship.
Here are some education stats added to the other day's vaccine correlation/COVID death analysis:
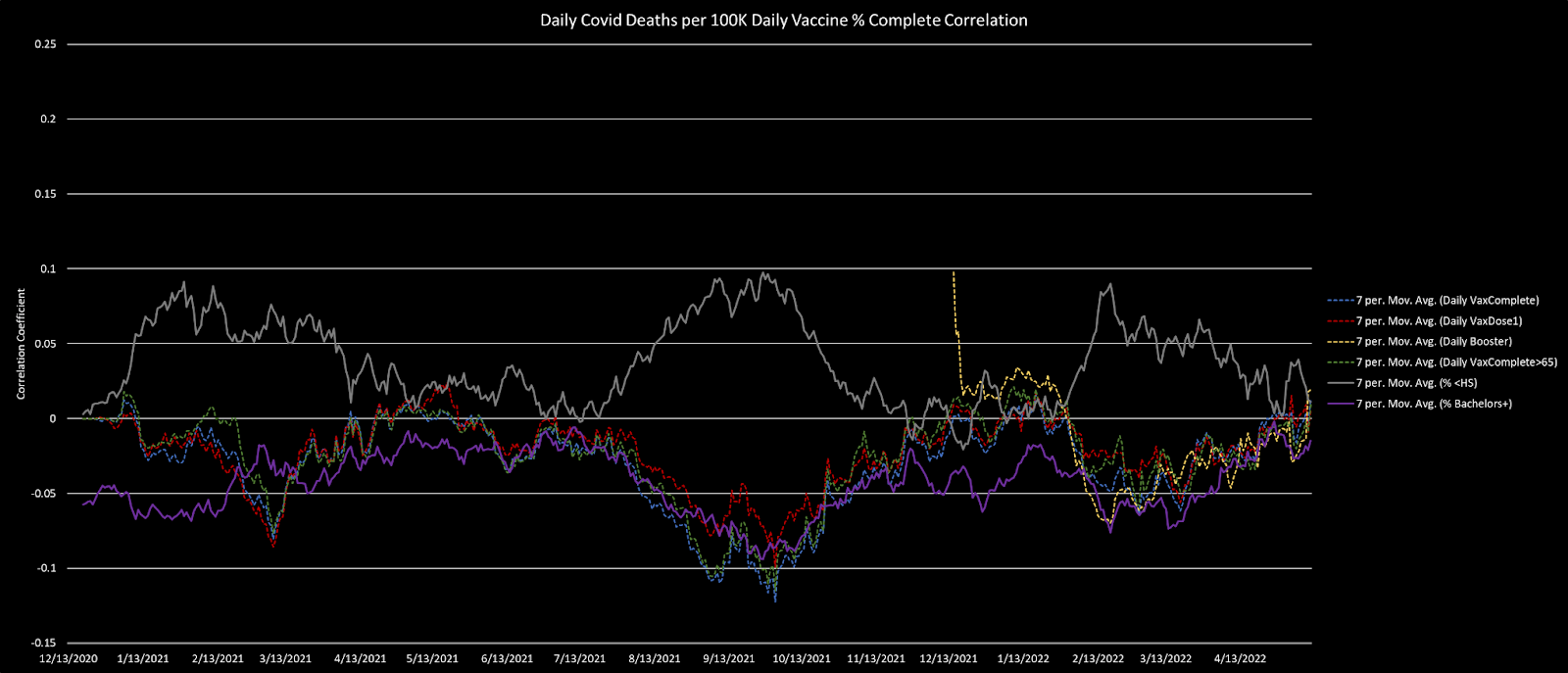
Whoa boy! There is a lot to unpack here.
First, we note that the vaccines are not at all the strongest correlates with mortality. But I'll take that a step further—it appears that education is more protective than vaccination.
Well, sort of. When we see correlations like this, what we should do is stop and wonder where the causation really lies. Are the experimental vaccines responsible for marginal advantages at the county level, or is education so responsible?
First, let us use our intuition: do you think that more educated people are more likely to know how to remain healthy?
That seems reasonable.
Okay. Do you believe that education leads to more income, and that people with more resources are likely to receive better healthcare?
If education did not lead to greater income for most people, it wouldn't be so popular. And if money could not buy better health, money wouldn't be quite so popular a pursuit.
It sounds like most reasonable people are on the same page. Thank you, mysterious voice…
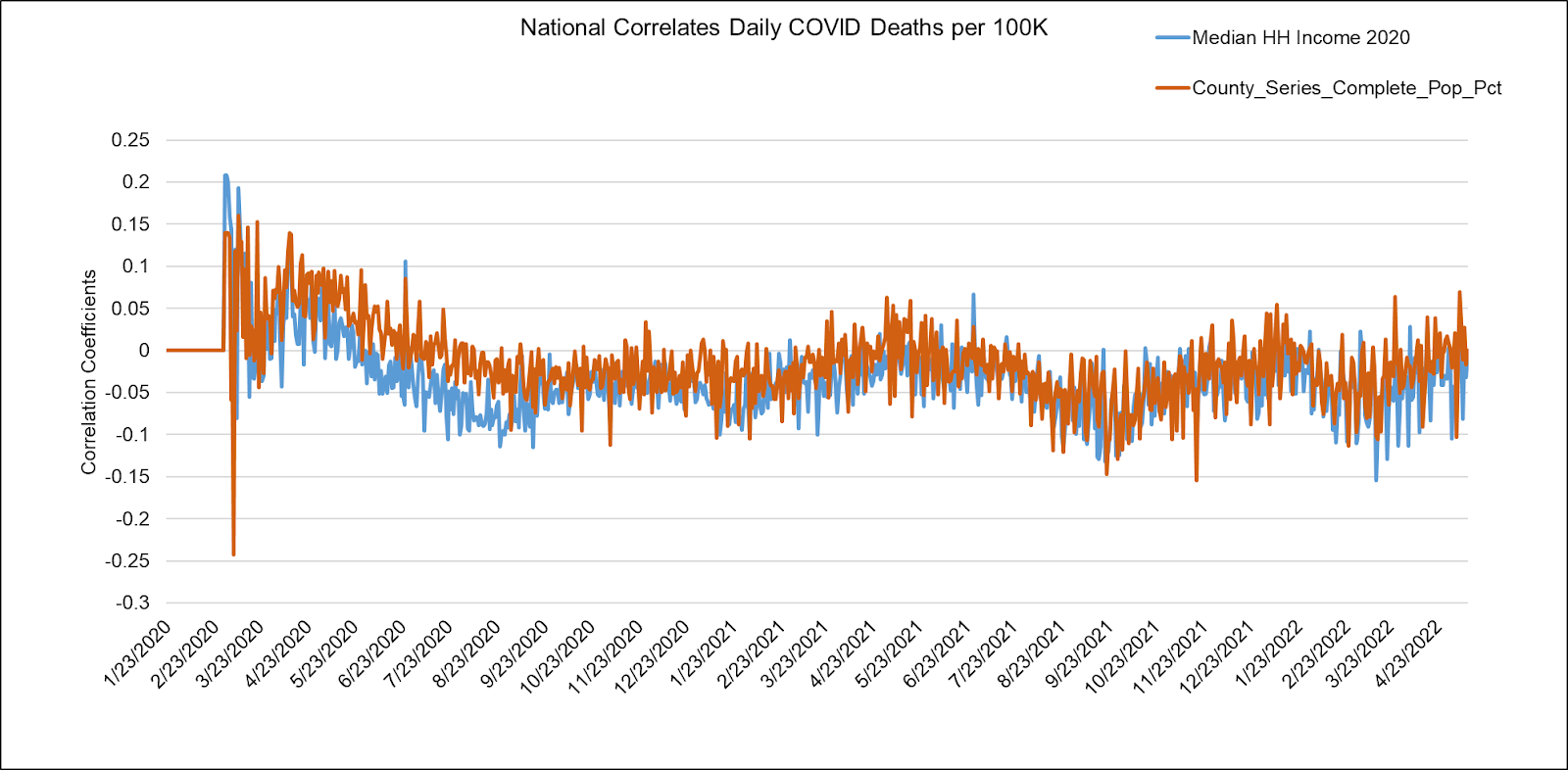
Once we made the leap to income, we find that after the very early stage of the pandemic, income is negatively correlated with daily COVID deaths, and almost perfectly tracks COVID case rates. This coupling happened prior to vaccine rollout and remained consistent since. Note that in the graph below, the correlations are to vaccination rates as of May 11, 2022.
Further, we can see the magnitudes of correlation between COVID-19 county income and education levels grow in a sustained way throughout the pandemic. These correlations are even stronger than the correlation between COVID-19 cases and deaths!
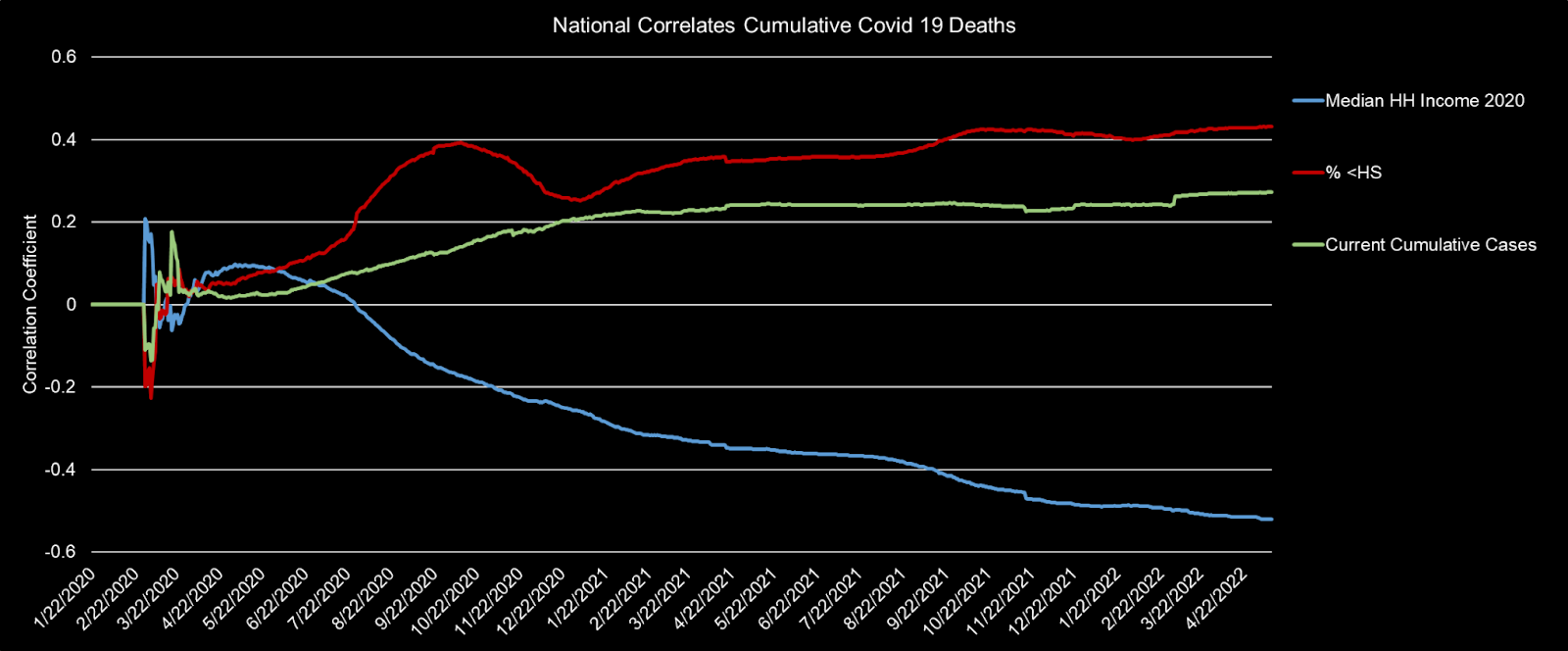
Think of the green (cumulative COVID cases, which are of course correlated with COVID deaths) as a basic sanity check. But also realize that any stronger correlation (which we see in the blue and red magnitudes) stands out as significant.
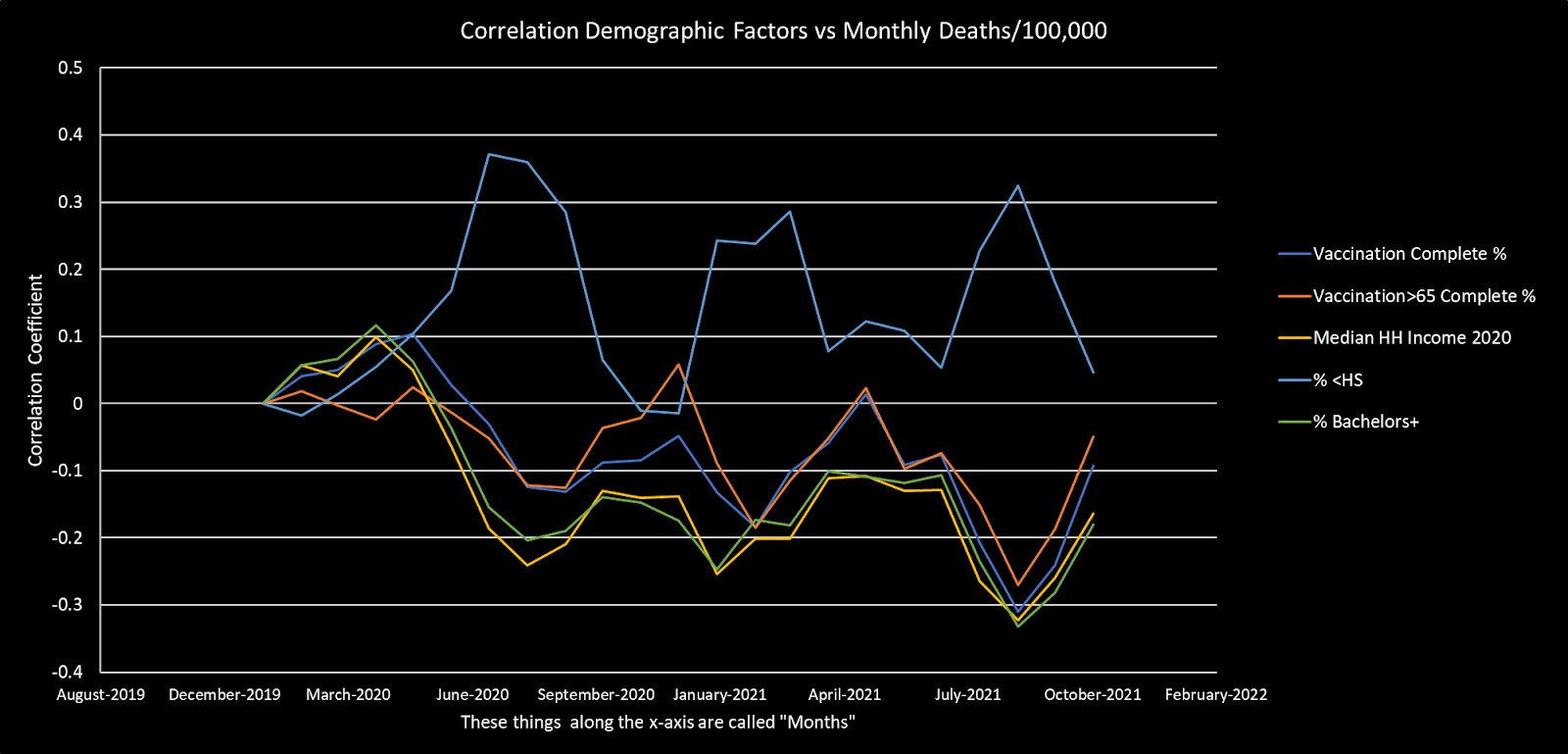
One more (from a prior article, so apologies that the black background misrepresents the graph by this article's rule) correlation chart: This is a month-by-month correlation analysis showing income and education trending almost in lock-step with vaccine rates in terms of their correlations with vaccination rates.
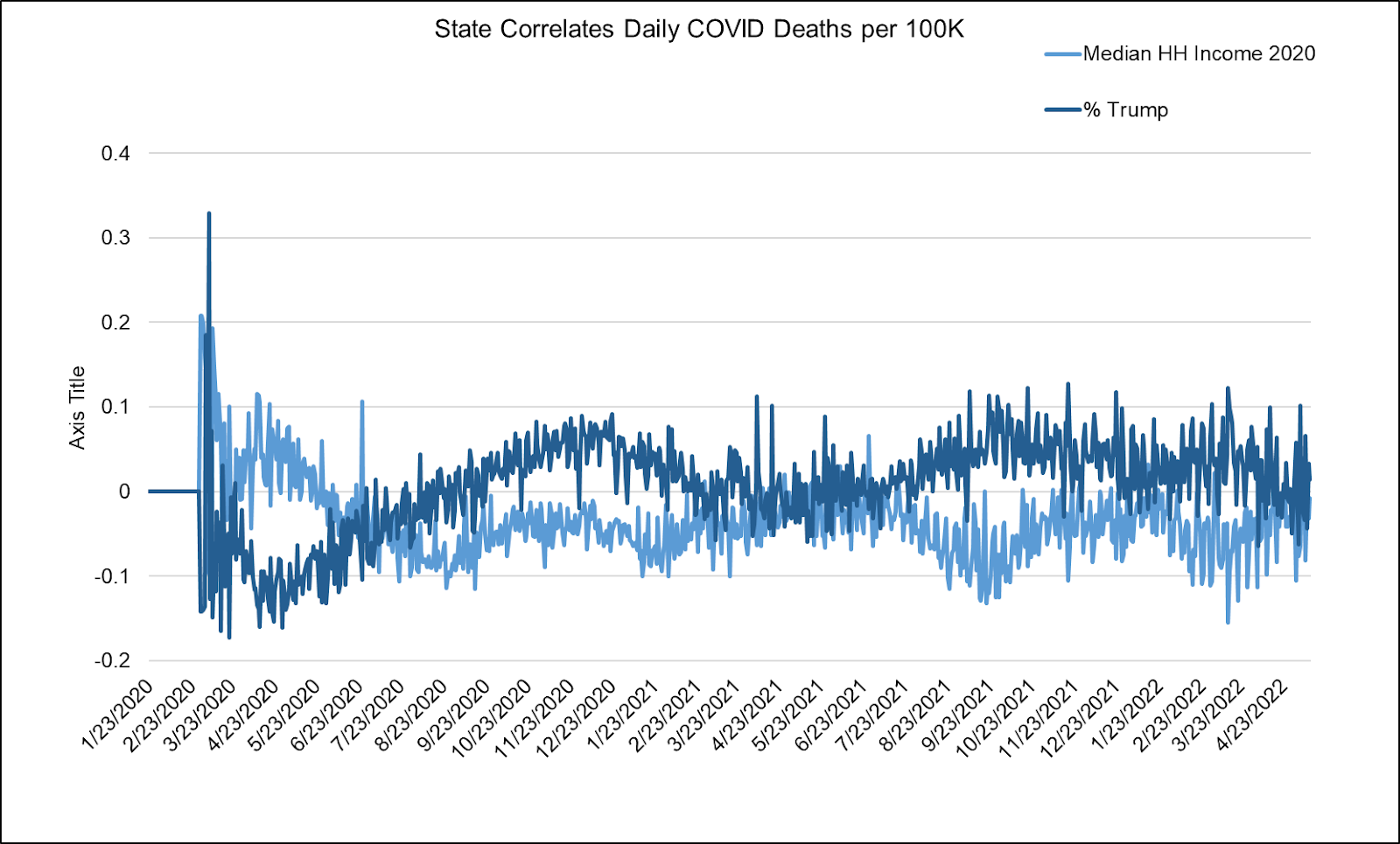
Further, when we isolate and compare income and voting effects on COVID-19 mortality, we find that partisan correlations are almost perfectly tracked by income. This makes sense unless you believe in some magical or yet-unearthed relationship between MAGA hats and ACE2 receptors.
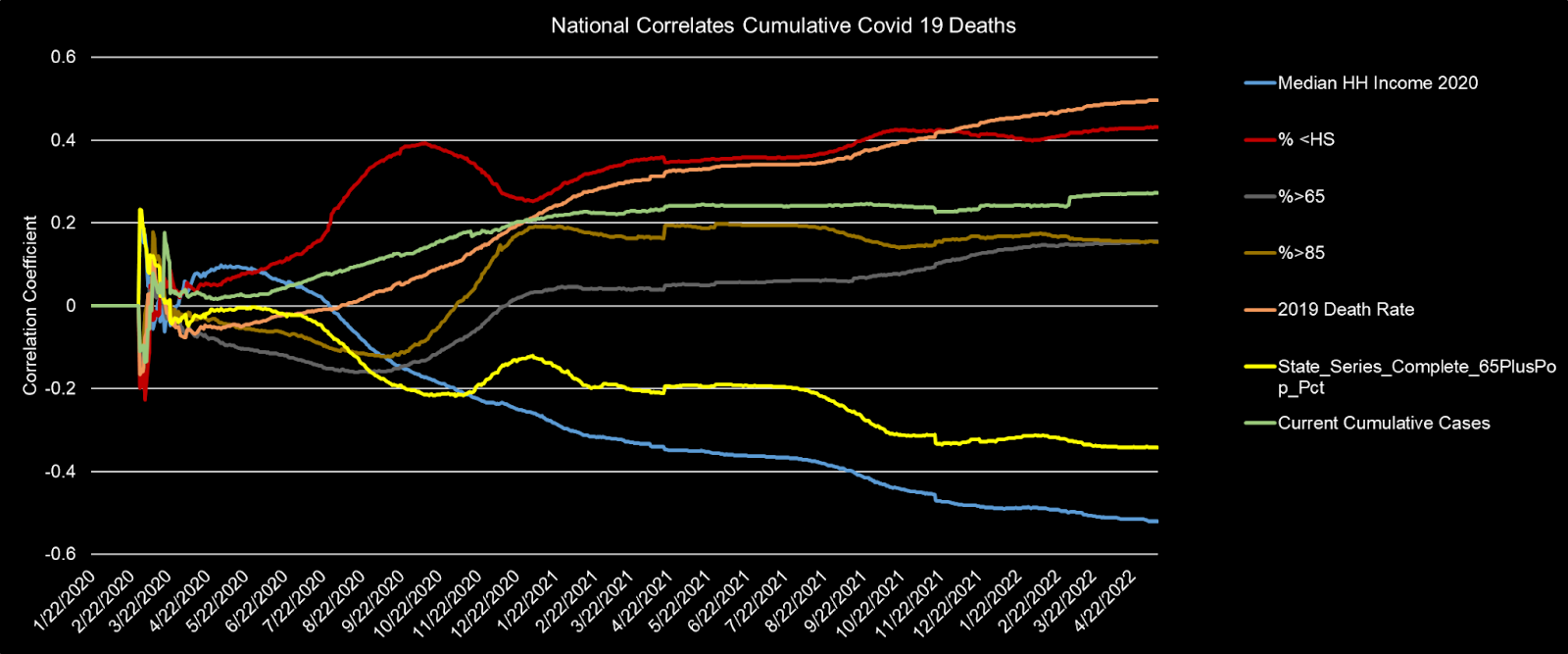
People Who Were Already Dying Revisited
Now that we've explored several relationships in the data, let's put some pieces together in the same charts. Here we see the strongest (magnitudes) of cumulative correlation (to COVID-19 fatalities) from (1) median household income, and (2) prior (recent) rates of all cause mortality (2019 specifically). These relationships are intuitively causal/correlated of health weakness on their own, but notably swallow up any mild appearance of efficacy (which would not appear mild if there were substantial VE).
Addendum: The Ethical Skeptic noted the same “VE is really just following prior mortality rate” phenomenon:


Mentally Ill/Disabled and COVID-19 Mortality
Warning: This section gets a little [more] disturbing.
There are several "hidden" comorbidities associated with COVID-19.
In April, researchers published a paper (Beaney et al, 2022) showing that mental illness and learning disabilities were more highly correlated with hospitalization and death than other factors, including socioeconomic deprivation.
We found significant variation in the case hospitalisation and mortality risk over time, which remained after accounting for the underlying risk of those infected. Older age groups, males, those resident in areas of greater socioeconomic deprivation, and those with obesity had higher odds of admission and death. People with severe mental illness and learning disability had the highest odds of admission and death. Our findings highlight both the role of external factors in Covid-19 admission and mortality risk and the need for more proactive care in the most vulnerable groups.
The mentally ill and those with lower cognitive abilities are often those without strong circles of support and advocacy. Together, with concerns over poor or abusive hospital practices, has led some to wonder if these patients are being picked on—perhaps a way of ratcheting up fear and compliance.

Please leave corresponding evidence in the comments. This post could be its own book with a true deep dive. But there is significant evidence for the CZVE hypothesis as well as the possibility that marginalized groups have been euthanized to create fear—perhaps to push people into the arms of history's largest medical experiment.
The first thing I think of when I think of higher education levels is higher income levels and lower economic stress. The laptop class did fine during the Covid lockdowns while the working class lost their businesses and incomes.
The Covid programs for really small businesses (not Harvard, which filed for relief as a small business, but my neighbors' little cafe) were a joke. My neighbors had to refinance their house and go through their lifetime savings to survive the year. In addition to their cafe, the husband had a contracting business doing displays, etc. for conventions. That business has never returned. He's now bartending at night while his wife runs their cafe. They feel like they will never be able to pay off their house or have savings again.
When I think of stress, the first thing I think of is the effects of stress on energy production. Specifically, stress hormones inhibit oxidative phosphorylation in favor of aerobic glycolysis. And aerobic glycolysis, which is cancer metabolism, is associated with bad Covid outcomes and every comorbidity associated with bad Covid outcomes.
"In severe cases, the cytokine storm is responsible for the most obvious signs of a COVID-19 infection including fever, lung injury which causes cough and shortness of breath (and the long-term complication, lung fibrosis) and in death. A causative factor related to the hyper-inflammatory state of immune cells is their ability to dramatically change their metabolism. Similar to cancer cells in many solid tumors, immune cells such as macrophages/monocytes under inflammatory conditions abandon mitochondrial oxidative phosphorylation for ATP production in favor of cytosolic aerobic glycolysis (also known as the Warburg effect)."
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7211589/
"Viruses usually target mitochondria as cellular power houses and various interplays have been detected between viruses and mitochondrial dynamics. Most viruses require aerobic glycolysis as the energy source for replication and its inhibition could attenuate this process."
https://onlinelibrary.wiley.com/doi/full/10.1111/dth.13810
And studies support that. Everything that inhibits aerobic glycolysis in favor of more efficient mitochondrial oxidative phosphorylation inhibits severe Covid-19, including Vitamin D, aspirin, niacinamide, progesterone, testosterone or DHT, and more.
High blood levels of polyunsaturated fatty acids are a specific feature of severe Covid. They also tend to be a specific feature of cancer and aerobic glycolysis instead of oxidative phosphorylation. In other words, they wreck your metabolism and energy levels. They hurt your mitochondria.
So I think higher Covid death rates among the working class are likely due to government policies like lockdowns. I think over the long run, though, that education benefit is likely to disappear or even turn into a disadvantage, as vax uptake was much higher among those with more education.
The only educated people with vax rates as low as the working class are science PhDs.
https://www.newswise.com/coronavirus/vitamin-d-and-lumisterol-emerge-as-cheap-and-easily-accessible-possible-treatments-for-covid-19/?article_id=757049
https://www.generalsurgerynews.com/In-the-News/Article/07-21/Aspirin-Reduces-the-Need-for-Mechanical-Ventilation-by-Nearly-Half-For-COVID-19-Patients/64048
https://www.biorxiv.org/content/10.1101/2020.04.17.047480v2.full
https://www.eurekalert.org/news-releases/659444
https://pubmed.ncbi.nlm.nih.gov/34661247/
https://www.nature.com/articles/s41598-021-90362-9
A lot to read there. Thanks. One issue I need to point out. Too me it's the elephant in the room. It's the data. Particularly the covid deaths, unless I missed it in your post that particular data is very corrupted. I'm not sure it can ever be corrected to some meaningful way.
First hospitals were paid to use covid as a revenue stream. When looking at the CDC deaths I am struck by the obvious errors. My favorite was the death by accidents yet counted as covid deaths. I guess that was a symptom of covid, falling in the kitchen and hitting your head. I can imagine the pressure docs recieved from the accounting side of hospitals to mark a death as covid if they were on Medicare; big paydays for each death. Another is death by some respiratory issue. This was a murky category, people die of respiratory issues every year, lots of them, maybe one of the largest category's. Yet that was mixed in with covid, how can you possibly fix this one and it was big.
The second issue for deaths is the manufactured death, yes it was real death but by the hand of ventilators and refusal for early treatment with older drugs. For instance, how many of the well educated band of data had more financial means could persuade a doc to use a banned medication that has been around for decades? We'll never know that number.
Once politics gets involved in a subject or issues it completely shrouds it in corruption, bias, and hell hole of the right left thing. The other corruption always lurking around political operations is money, big profitable opportunities were everywhere with this plandemic, far more than we realize.
So you see while this hard work you put in is impressive and we are grateful for, it has to be framed in some unprovable (at least for now) caveats that may greatly change the interpretation.