


Mechanistic Evidence of Vaccine-Induced Mortality
The Chloroquine Wars Part LXXV

"A hallucination is a fact, not an error; what is erroneous is a judgment based upon it." -Bertrand Russell
Debates over causality in biomedical data are poorly framed. The fact of the matter is, causality cannot ever rise above the level of opinion (until such time at which all the mysteries of the universe are unraveled, which seems exceedingly unlikely in the age of "Trust the Science"). Criteria such as Bradford-Hill are not what guides most doctors and scientists who often form opinions based on some subset of those or other criteria because any evidence is better than no evidence. But weaker opinions turn to stronger ones when the evidence suggests a mechanistic picture, however we check the criteria boxes.
The Evidence Comes Together
We already have plenty of evidence painting a picture of a great deal of COVID-19 and vaccine-associated injury caused by the spike protein (here and here). Recent research (Patterson et al, 2021) suggests long haulers have a hard time exercising until spike protein filters from the body, which dovetails into evidence we discuss below. In this article, we discuss the addition of both dose dependence and delivery dependence of damage associated with mRNA inoculations (Pfizer and Moderna) to the evidence pool. As we continue, ask yourself what evidence would move your needle [of judgment] toward a likelihood of substantial vaccine-induced mortality if all of this does not.
In a paper published on August 18 (Li et al, 2021), researchers examined the effects of mRNA vaccine delivery in an animal model. The results are profound, sometimes demonstrative, and sometimes subtle. My list of concerns may span several articles. This study alone condemns continued human experimentation. It contributed to a body of evidence that will hopefully be instructive for generations as to why never again to jump past basic safety experiments in the balance between the desire for a solution and reasonable costs paid in achieving it [to a problem barely felt on the level of the global population].
What seems particularly sad about all this is that there are so many other solutions from early treatment medicine, to intentionally inoculation with less harmful coronaviruses, to nasal sprays, to less risky vaccines.
Dose Dependence
There are few better gauges of mechanistic causality than dose dependence. Certainly, every variable or metric can fool us at times, but dose dependence is one of those signals that fools us rarely.
The Li paper shows dramatically elevated and dose dependent markers for auto-immune reactions, inflammation, and cardiac damage. Such effects are a large subset of the problems central to the debate over the vaccines. This evidence further points toward my suggestion that we should be opening wider the etiology of COVID-19 to include vaccines that contain or produce the spike protein. Simply understanding the definition of disease helps us better analyse the problem.
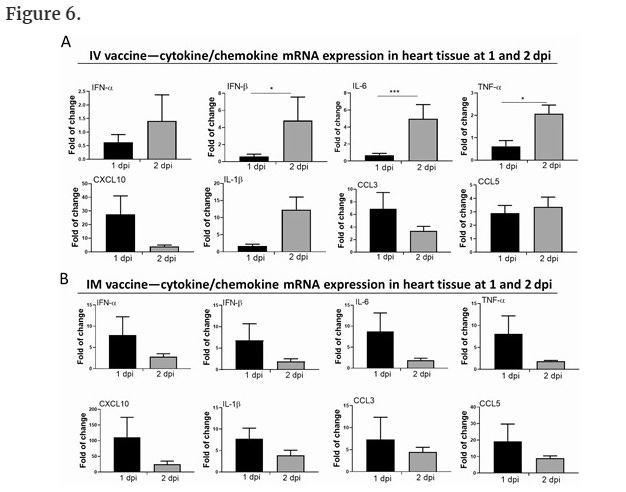
Delivery Dependence
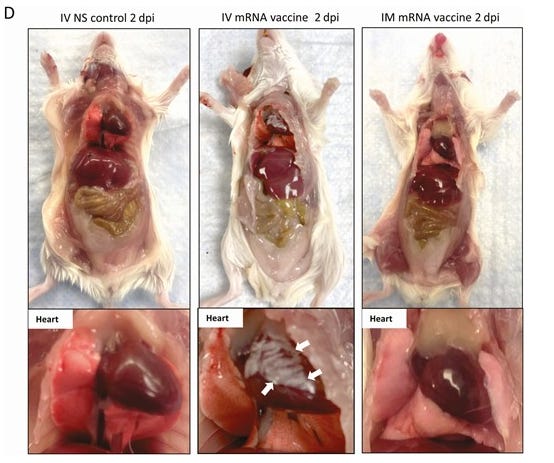
In addition to dose dependence, the Li paper reports on experiments that vary the delivery mechanism of mRNA vaccines. The cohorts include a control group of rats, a group where mRNA inoculation was delivered to the muscle, and a group in which mRNA inoculation was delivered intravenously to the bloodstream.
It is now well established that COVID-19 vaccines cause myocarditis and an array of related cardiac problems. In the six month Pfizer report, cardiac mortality skewed substantially toward the vaccine arm. In the Li paper, we see profound impacts to the hearts of rats that had either dose of mRNA vaccine injected into the bloodstream. Occam's razor pushes us toward a presumption that mRNA vaccine in the blood results in cardiac damage (and perhaps other issues such as clotting).
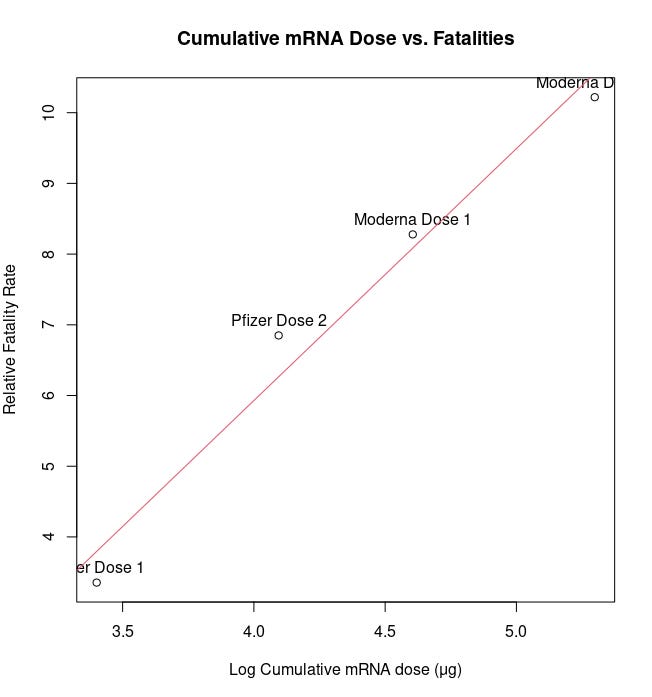
Just today, quant Kamal Mokeddem posted a compelling correlation analysis between lognormalized mRNA dosage and VAERS fatalities. The fit is stunningly perfect (R^2 = 0.97, p = 0.0137). Such a strong fit also strongly suggests that the proportion of the VAERS deaths (for COVID-19 vaccines) associated with background mortality is very likely quite low. This flies in the face of arguments made by vaccine partisans who, without pointing to any study of the bodies, suggest that most or nearly all of the VAERS deaths are coincidental and unassociated with vaccination. That quants outside the biomedical field are engaging an issue such as this one more than nine months into an experimental mass vaccination campaign strongly indicts vaccine manufacturers, academics who should be playing watchdog, and the entire American public health system.
It is noteworthy that the greatest incidence of myocarditis and similar ailments is among men under the age of 30 and teenage boys. This is exactly the population you would expect to be building more muscle mass, requiring greater blood circulation to muscle tissue. Reporting of these cases is still growing.



I have to wonder if those people approaching their physical peak have greater blood circulation through their muscle tissue, resulting in greater likelihood of carrying spike protein throughout the circulatory system. The Li animal model study and others such as Payvandi et al (2021, N = 30) do not include enough individuals to observe whether 1% or 0.1% or 0.01% of the vaccinated population (intramuscular injection) are likely to see mRNA create spike protein that leaks into the blood. And the lack of any all-cause mortality benefit in the six month Pfizer study is direct evidence that however strong this effect of spike protein toxicity might be, it seems to be enough to entirely reverse all mortality benefits for the vaccines---and that's long before we include mortality estimates, or see all the other serious adverse events play out over the next few years.
Supportive Evidence
Research (Annie et al 2021) suggests three times the risk of COVID-19 death among those with myocarditis than those without, among those infected with SARS-CoV-2. And having myocarditis likely increases the chances of iatrogenic infection by a large degree (perhaps the FDA and CDC should be studying this?). While we may not yet have enough information for a complete comparison of spike protein-associated myocarditis with the broader superset of myocarditis etiology, we should note the severity of the condition is high. In one study (Kuhl et al, 2012), those suffering from myocarditis had 75% and 44% survival rates at 3 to 10 year time frames. If this rate holds, even 40 cases of myocarditis per million doses roughly results in an additional 10,000 deaths among mostly young people over the next decade. This is itself many times more than the roughly 4,000 Americans under the age of 30 who have died with COVID-19, almost none of whom died primarily due to COVID-19.
That estimate might be conservative. My friend, Jessica Rose, PhD, who presented at the recent Vaccines and Related Biological Products Advisory Committee, recently published a paper (Rose, 2021) that includes an estimate of over 20,800 cases of myocarditis. In a conversation we had, she agreed with my suggestion that her underreporting factor of 30x is likely a floor of the real number since it is derived from the 0.7% incidence of serious adverse events in the Pfizer and Moderna trials. These studies included mostly healthy individuals, and few elderly, whereas distributions of SAEs in VAERS lean heavily toward the elderly.
There may be good reason to believe the number will be higher. There are debates that suggest subclinical myocarditis rates could be an order of magnitude or more higher than current tallies. Might we see 20,000 young American lives cut short over the next decade due to these sparsely-tested gene therapy interventions? Could the number grow into the hundreds of thousands in 20 or 30 years? What about worldwide?
The following video made by Dr. John Campbell examines injection technique related to the potential for harm.
I don't mean to get partisan (I don't vote as a partisan), but I wonder how Dr. Campbell would rate this delivery on a safety level.

How do they get away with opening with:
Safe and effective whole-population vaccination against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is the only long-term solution to the ongoing coronavirus disease 2019 (COVID-19) pandemic [1]
The only long-term solution?
This study does not show that, let alone prove it, yet it's in there as a fait a compli.
Not sure if you've seen this study on myocarditis following smallpox vaccine, but it is amazing in its parallels
"The myocarditis/pericarditis incidence rate for the post-SPX cohort was 463 per 100,000 (95% CI 150–1079 per 100,000)."
"...when compared to the published background rate of MP in a comparable population of service members not exposed to SPX immunization (detailed in Table 3)[3], the relative risk of clinical MP was 214 fold higher (95% CI (65–558); p<0.001) than the published background rate. "
"Prior to the present study, the incidence of MP following smallpox vaccination was estimated from passive surveillance registries and population databases, with an inherent bias towards underestimation of disease incidence. "
Engler RJ, Nelson MR, Collins LC Jr, et al. A prospective study of the incidence of myocarditis/pericarditis and new onset cardiac symptoms following smallpox and influenza vaccination. PLoS One. 2015;10(3):e0118283. Published 2015 Mar 20. doi:10.1371/journal.pone.0118283-2198(21)00702-9.