


How Flu Vaccines Accidentally Reveal the Efficacy Illusion
Shattering the Efficacy Illusion, Part 9

Articles from the Vaccine Wars can be found here.
Hat tip to Dr. Irene Mavrakakis, of whom I just recently became aware. While I honestly do not know if this tweet is meant tongue-in-cheek, she made me aware of the important information.

The paper cited by Dr. Mavrakakis (Wolff 2020) is a study on military personnel, which is itself interesting in light of all the evidence that there is some sort of association between the U.S. military and vaccine production. I keep thinking back to Dr. Robert Malone's statement that the flu vaccines were understood (by insiders) not to work, but were kept in place as a way of ensuring mass manufacturing capacity in the event of a bio-disaster.
The researcher makes a leap in the paper without respect to other hypotheses.
Results
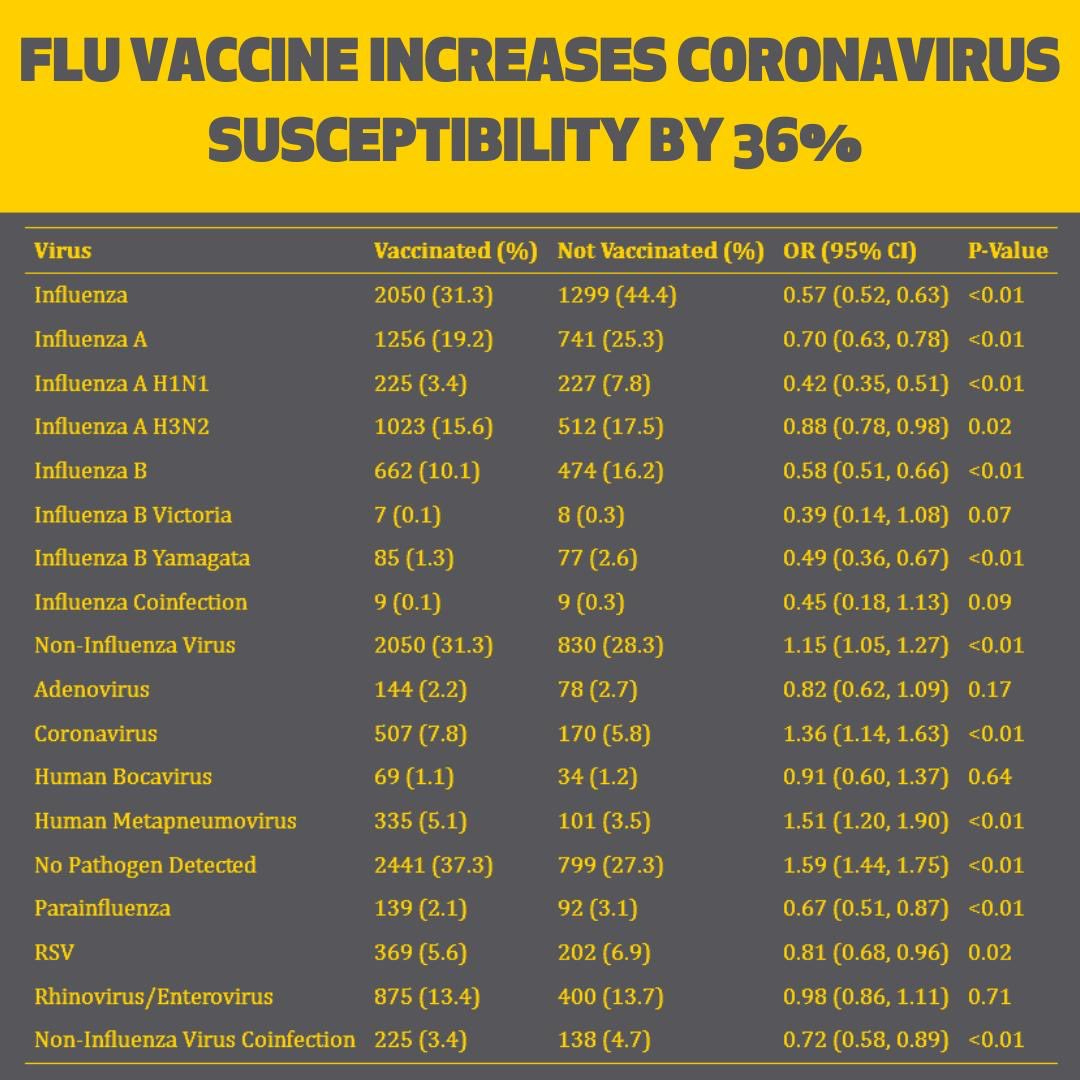
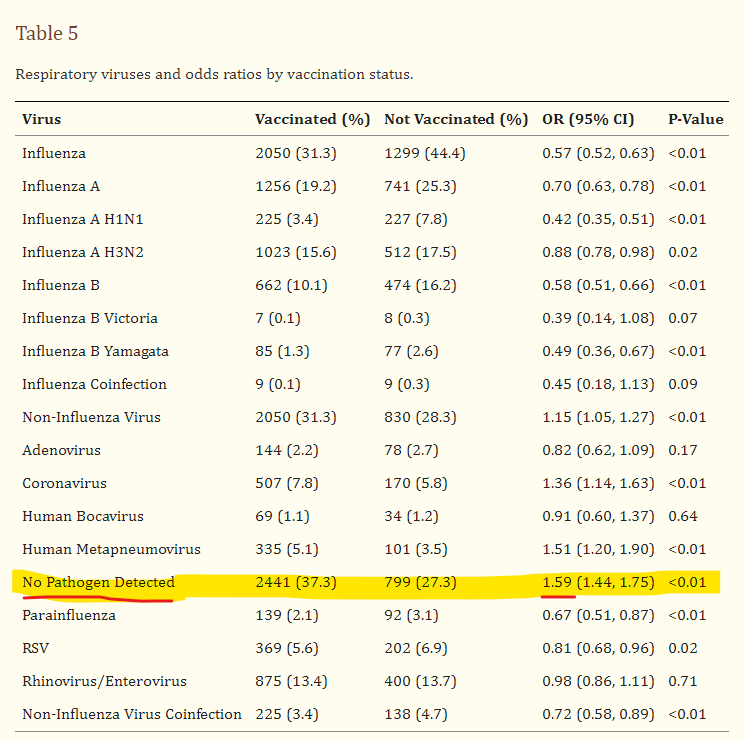
We compared vaccination status of 2880 people with non-influenza respiratory viruses to 3240 people with pan-negative results. Comparing vaccinated to non-vaccinated patients, the adjusted odds ratio for non-flu viruses was 0.97 (95% confidence interval (CI): 0.86, 1.09; p = 0.60). Additionally, the vaccination status of 3349 cases of influenza were compared to three different control groups: all controls (N = 6120), non-influenza positive controls (N = 2880), and pan-negative controls (N = 3240). The adjusted ORs for the comparisons among the three control groups did not vary much (range: 0.46–0.51).
Conclusions
Receipt of influenza vaccination was not associated with virus interference among our population. Examining virus interference by specific respiratory viruses showed mixed results. Vaccine derived virus interference was significantly associated with coronavirus and human metapneumovirus; however, significant protection with vaccination was associated not only with most influenza viruses, but also parainfluenza, RSV, and non-influenza virus coinfections.
The other hypothesis that should have been considered is that the flu vaccine somehow made recipients more susceptible to several other viruses—including coronaviruses. Instead, Dr. Wolff aggregates the effect of flu vaccines on influenza infection with non-influenza infection—a clearly interesting bifurcation of categorization and results—and comes up with a 0.97 odds ratio, and says, "no effect".
Huh.
While Dr. Wolff might have dismissed the [bolded] alternative hypothesis, he should not have done so without commentary. But what if a mechanistic relationship between flu vaccination and coronavirus infection had not gone unnoticed by the military or vaccine makers?
(Note: The possibility that flu vaccines make recipients more likely to be infected by a coronavirus would apply just as well to infectious clones of coronaviruses.)
How Should We Interpret the Wolff Paper?
First, note that those who received flu vaccinations were overall less often infected with the various viruses tested.
As I have previously discussed, there are some researchers who see this phenomenon for the first time and wonder, "Maybe one vaccine somehow helps the immune system fight completely different viruses." Were that true, we would find such effects after recovery from viruses as well, and the effect would be well-documented (and named). While I'm a general statistician, not a biostatistician, I suspect that I would have heard of such a relationship after 30 months of reading and computing vaccine statistics.
(Yes, I've heard discussion of hypothetical connections between vaccination for one disease and immunity to another, but have I not discovered or been presented with convincing evidence.)
What we do see is almost certainly another observation of the Healthy User Bias (HUB).
Now, look at the subset of viruses listed that vaccine-takers were more likely to catch.
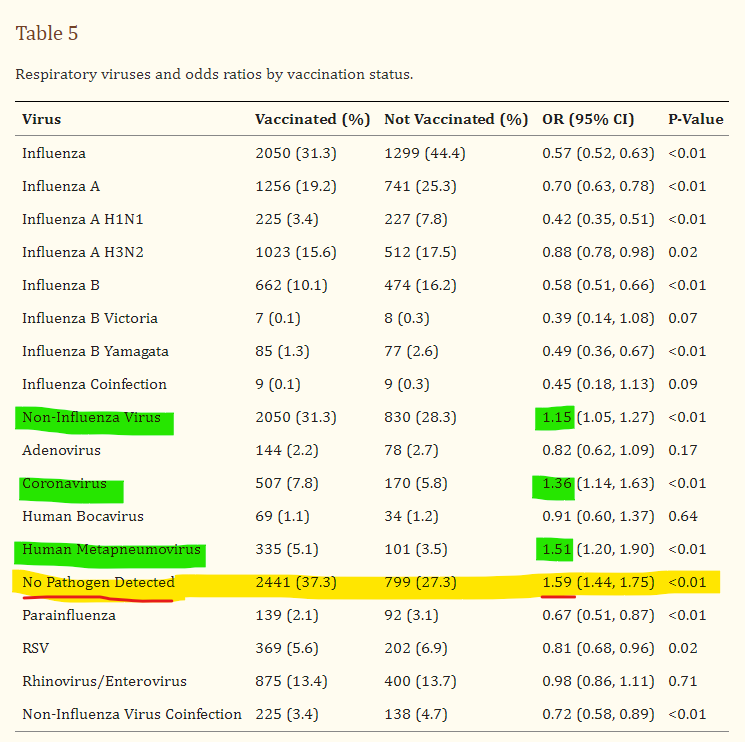
Coronavirus and human metapneumovirus. You may have noticed metapneumovirus suddenly in the news over the past couple of years.

It turns out that along with RSV and parainfluenza, metapneumovirus exploded in prevalence during the COVID-era, just after the rollout of the COVID-19 vaccines.
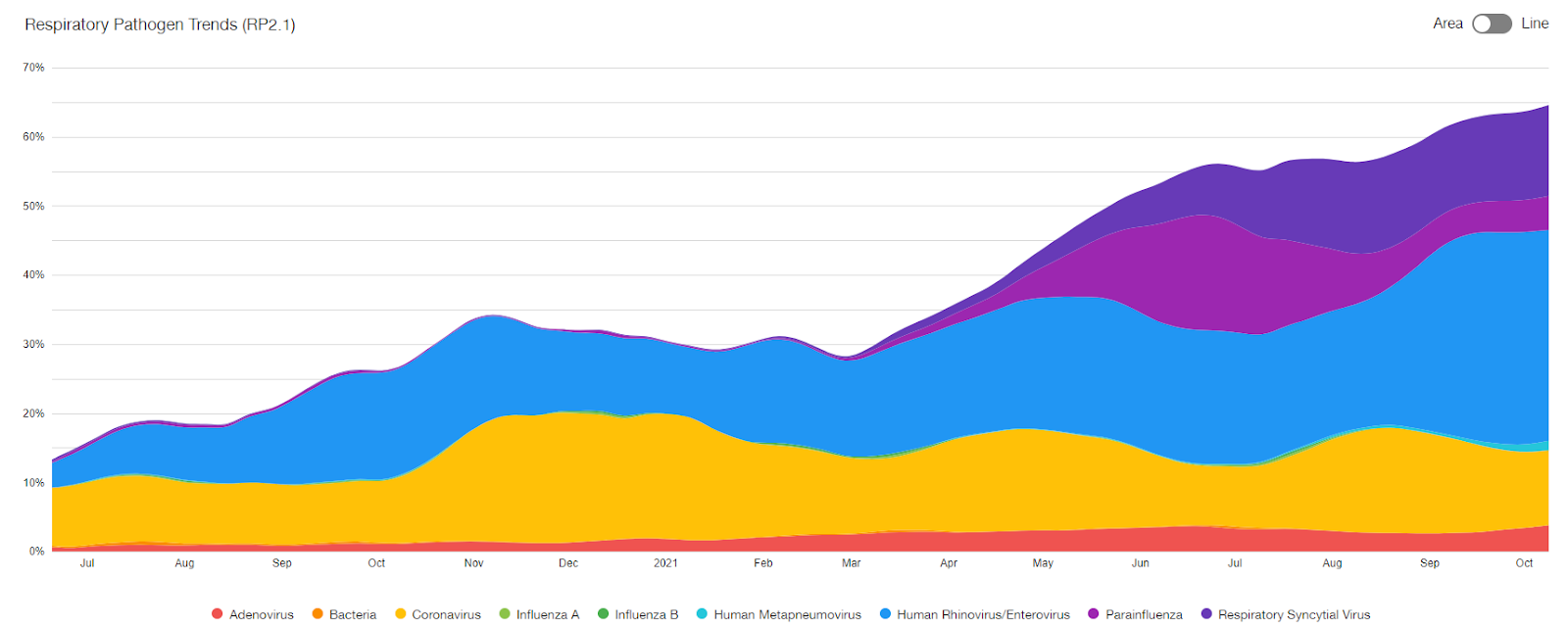
While you might notice that RSV and parainfluenza grew from almost non-existent levels, metapneumovirus prevalence doubled during the first few months after COVID-19 vaccine rollout.
Military Knowledge of How to Spread COVID
Clearly, this is circumstantial evidence, but what we can conclude is that smart people in the military-industrial biowarfare complex had data prior to the plandemonium about how to create a vaccine that would result in higher levels of coronavirus infection. On its own, I wouldn't think too hard about this revelation, but in light of all the other evidence that at least some portion of the military-industrial complex is in control of the experimental COVID-19 mass transfection program, I take this observation more seriously as a piece of confirmatory evidence.
The phenomenon of vaccines protecting against other infections is called non-specific effects (NSE's). This is usually discussed in the context of childhood vaccines in low-income countries, and is basically always used to describe benefit rather than detriment, though it can apply in both directions. Sometimes the term off-target effects is used. The studies are typically very confounded and consumed by society unintelligently. However, some beneficial NSEs are probably real. This would be BCG vaccine and also live oral polio vaccine. (OPV). In the case of OPV, this is demonstrated with a natural experiment, meaning comparing childhood mortality in a region just before and after introducing the vaccine. This avoids the usual confounding as you are in essence comparing a society to itself at different times, rather than comparing vaccinated to unvaccinated people. Two similar natural experiments are among the studies which implicate DTwP vaccine in increasing childhood mortality. Same of some other vaccines as well. Some vaccines do not have data available to do such natural experiments.
Continued vaccine injections will result in the extinction of human beings from earth.