


Defining Away Vaccine Safety Signals 6: DMED Revision, Medium Resolution
The Vaccine Wars Part XXVIII

We need for members of Congress and other American leaders to put the DoD's feet to the fire over this. We could be witnessing the sabotaging of the U.S. military, and leadership at the DoD either needs to swiftly investigate now, or else we should assume that manipulation of health data for the purpose of hiding harms due to experimental gene therapy injections to be intentionally directed at harming brave members of the U.S. Armed Forces. This did not need to happen, and it does not need to continue.
Find a way to take action. I am a private person who intended to remain under the radar for my entire life. I am now looking into speaking in court, in medical policy meetings (more about that later, but I don't want to tip my hand), and possibly in Congress from the position of a dissident. This moment is that important. Find your way of participating in holding criminals accountable, and in making greater peace and prosperity out of the future. Otherwise, the America that we have going forward is the America that the criminals want to sculpt it to be (and it has been more that way for longer than most Americans are willing to admit just yet).
While researching the DMSS/DMED numbers, I was told by a ranking member of the U.S. military that this extremely important health data for the U.S. military is in fact exported outside of the United States (to Israel) prior to the data being passed from the DMSS to the DMED. If true, I find it mind boggling. How could this data not be viewed as a national security interest? What added value from a foreign source could outweigh the risks associated in allowing foreign agents or governments (and we should assume the capture of that information by government) to handle, much less document, the data that tells the U.S. military the readiness levels of the troops?
Where Were We?
Recall where we were, previously.

That article lays out a great case for fraud taking place at the point of publication of the May 2021 MSMR. This article should be seen as a companion to that one, laying out a more complete picture of what the data looks like. This article will not focus on 2021 data, but rather the 2016 through 2020 data to get a better understanding of what the data manipulation looks like. I will use this as a reference in future articles, but also for arguments made that will be sent to Congress via Thomas Renz.
We will be examining a lot of charts such as the one below, so let's talk about how to read it.

The grey bars show summary ambulatory data originally reported in May edition MSMRs prior to 2021. My strong opinion is that this is true data (prior to what looks on face like massaging of the data for the May 2021 report).
The red bars show summary ambulatory data as published in the May 2021 MSMR.
The blue bars are the results of queries performed from DMED in February, 2022.
Trend lines (dotted at the top) are not critically important for this article, but advanced chart readers may find maintenance of trends or changes in trends to be interesting. But every reader can look at the trends and ask, "Does 2020 look like there was a health crisis?" No. No, it does not.
Initial Observations
Some of this is a repeat from the last article, but we're about to show a lot of these charts, so if you're interested, now is the time to really get a grip on what we're seeing.
For all 2016 and 2018 comparisons, the red/blue bars are elevated from the prior published data in grey for every single major diagnostic category reported. We leave out the "Other" category that underwent redefinition.
For just one major diagnostic category, the blue bars are elevated above the red bars. We will talk about the importance of the difference.
We are examining large collections of different illnesses in the diagnostic categories that follow. There are thousands of ICD-10 codes within each of these categories. There may be 2%, 45%, and 700% changes in incidence of illness or injury for various ICD-10 codes or collections thereof that describe a specific disease, whereas the change for the overall diagnostic category may be 4% or 12% or 30%, depending on how it all balances together.
A large change of rate in an illness with a low rate of incidence may barely impact the change of rate in illness over the larger diagnostic category.
I hope I've made this list plain enough. You can look back here if need be.
The following ordering of the categories is essentially from the greatest incidence (in terms of ambulatory reports) to the least. Many of the more interesting categories are near the bottom.
Musculoskeletal System and Connective Tissue (ICD-10: M00-M99)
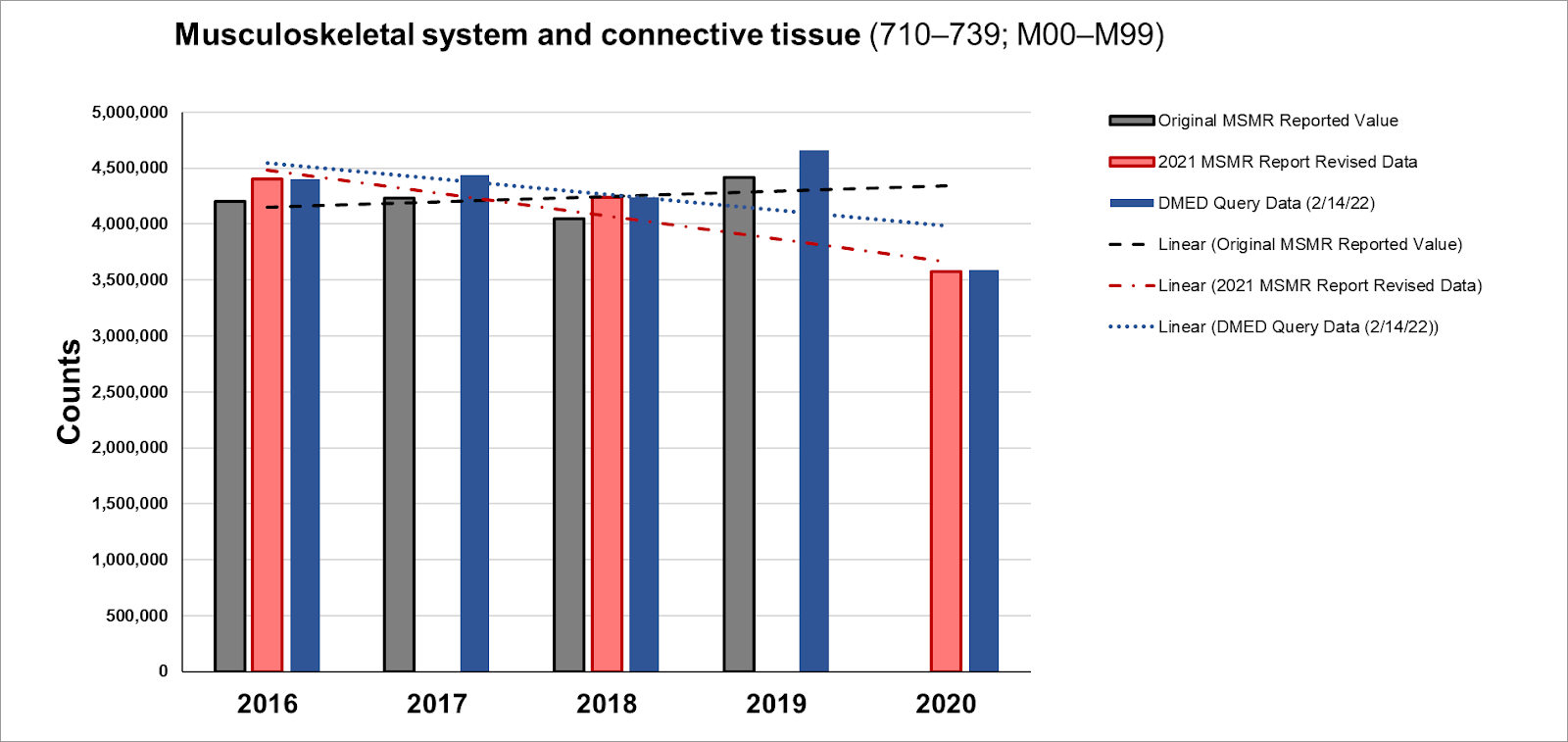
The 2016 and 2018 summary ambulatory data were upwardly revised 4.5% and 4.9%, respectively in this large category. This is one of the smaller changes among the major diagnostic categories, which is consistent with observed distributions of vaccine-associated illness.
Mental Health Disorders (ICD-10: F01-F99)
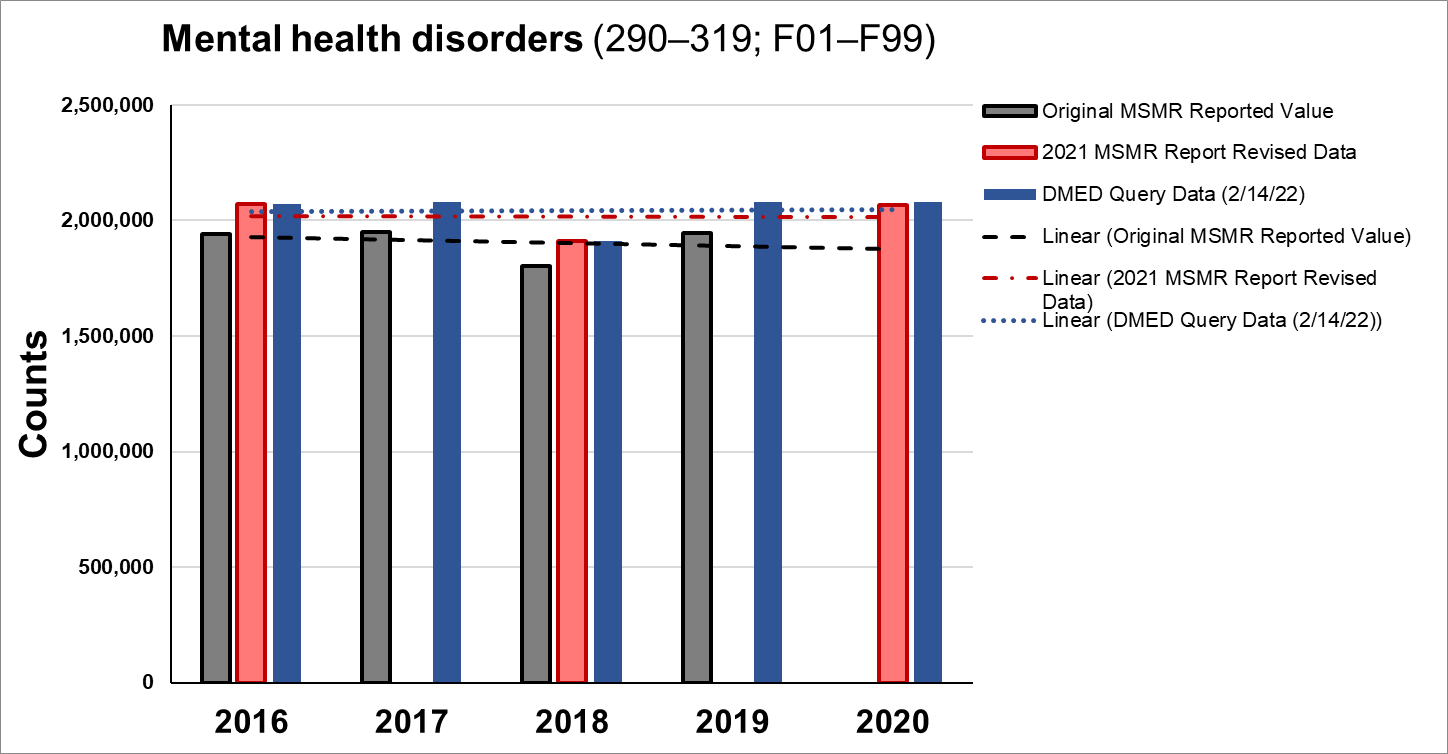
The 2016 and 2018 summary ambulatory data were upwardly revised 6.5% and 6.2%, respectively in this large category. This is one of the smaller changes among the major diagnostic categories. Personally, I view the observed rise in mental illness as primarily related to the stress that terrible and terrifying policy has placed citizens under, including the psychological nudges.
Nervous System and Sense Organs (ICD-10 Codes: G00-G99,H00-H95)
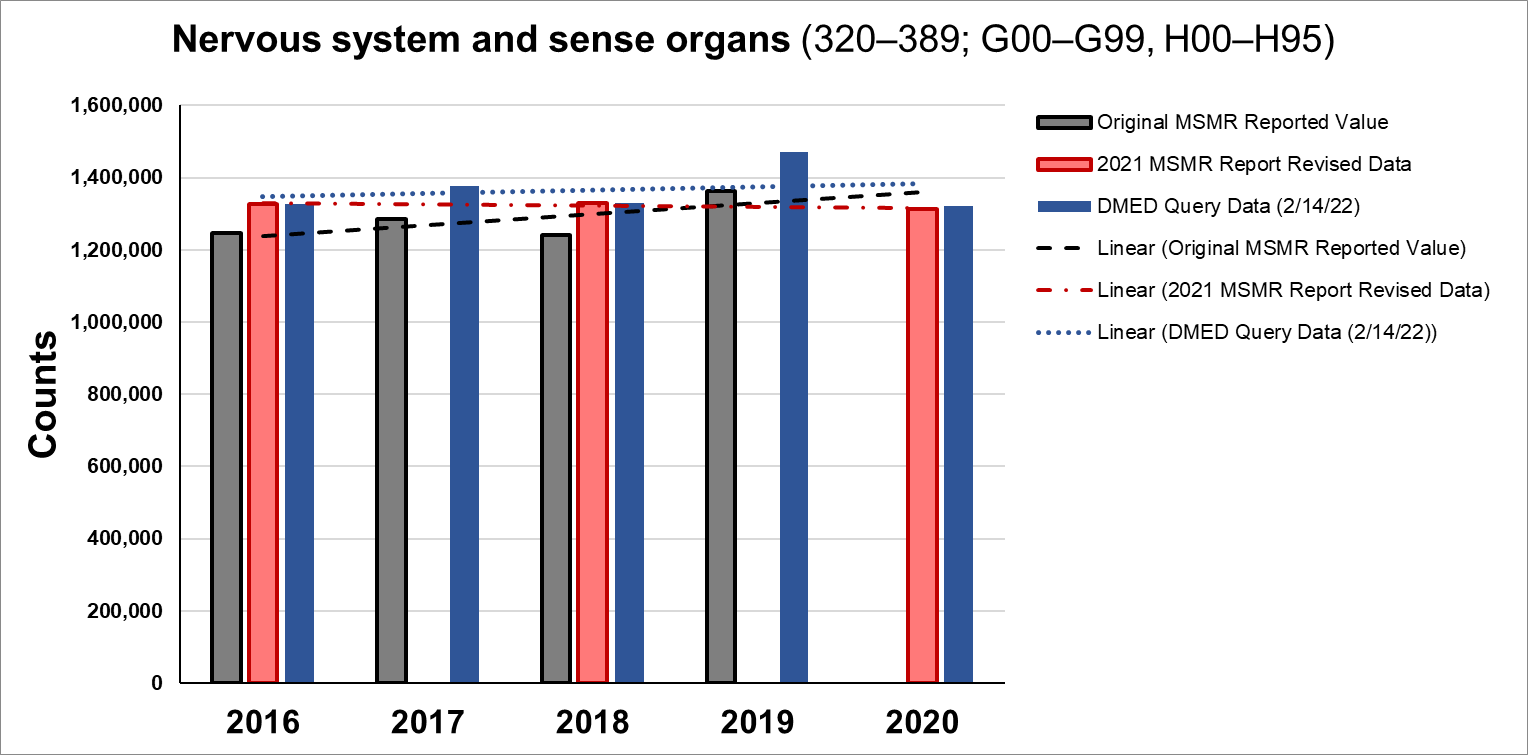
The 2016 and 2018 summary ambulatory data were upwardly revised 6.5% and 7.2%, respectively in this large category. This is still a smaller than average change, but to a large enough category that zooming in may prove interesting.
Signs, Symptoms, and Ill-Defined Conditions (ICD-10 Codes: R00-R99)

The 2016 and 2018 summary ambulatory data were upwardly revised 11.7% for each year in this diagnostic category. This may prove to be the most interesting diagnostic category. Most major diagnostic categories tend toward correlated disease expression. In this category, diseases and injuries are themselves not the important aspect. These codes are defined by cases in which the etiology is in question. This would be a place where we should expect to see physicians either confused about what a vaccine injury represents or not wanting to state with certainty or believe that a particular vaccine injury is an injury. I talked about this previously, but the second revision of the 2016-2020 data, which is quite large (46.6% on average), looks suspiciously like cover for dramatically higher rates of illness tossed into this bucket.
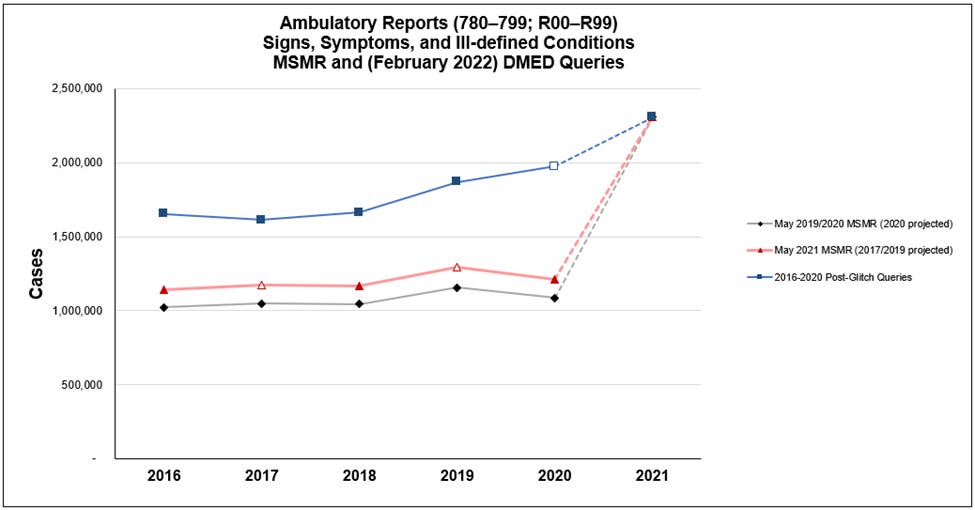
The post-glitch queries look molded to indicate a trend was already taking place. But there is no such pre-pandemic trend in any other data I've looked at (outside of military database outputs), much less in the other major diagnostic categories.
Some of these categories are likely matches for effects of the quasi-vaccines, and there are many more that do aside from the list below:
(R01x) Cardiac murmurs and other cardiac sounds
(R03x) Abnormal blood-pressure reading, without diagnosis
(R04x) Hemorrhage from respiratory passage
(R07x) Pain in throat and chest
(R09x) Other symptoms and signs involving the circulatory and respiratory system
(R22x) Localized swelling, mass and lump
(R77.1) Abnormality of globulin
(R77.8) Other specified abnormalities of plasma proteins
It may also be that cases categorized as R-codes get recategorized down the road as etiologies are better understood, so illnesses that currently show no increase or modest increase in rates in 2021 could wind up showing substantial increases as the dust settles.
Expect me to have a lot more to say about the R-codes down the road, and with as much resolution as we can get.
Injury and Poisoning (ICD-10 Codes: S00-T98; DoD0101-DoD0105)
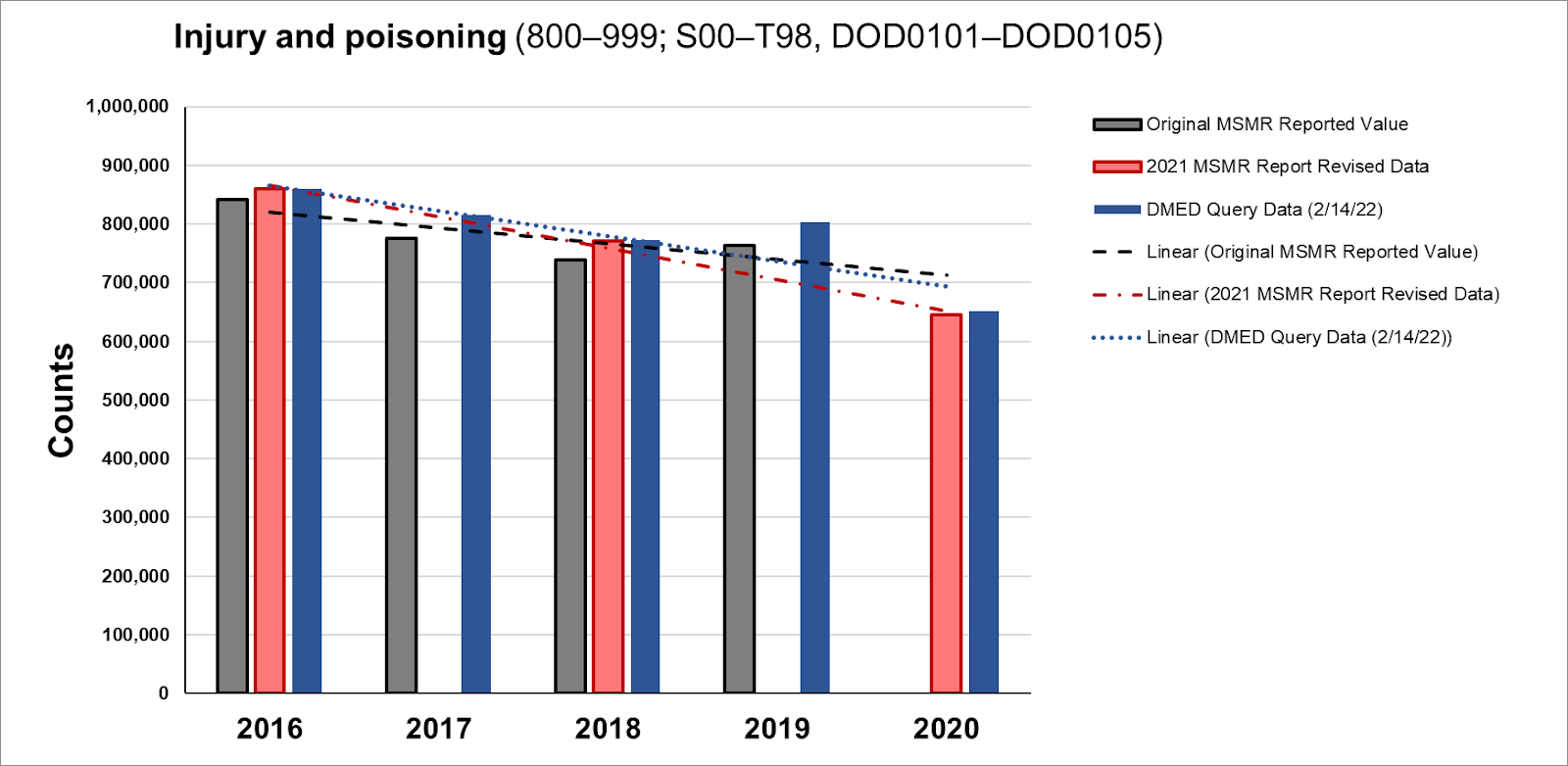
The 2016 and 2018 summary ambulatory data were upwardly revised 3.7% and 4.5%, respectively in this diagnostic category. My priors are that we will only find interesting stories in this data when we drill down for higher resolution, so not much to say for now. However, this category does include a couple of key ICD-10 codes with respect to vaccinations.
There are over 2,000 reports of severe adverse events among military personnel in VAERS, which is a database notoriously underreported by factors as high as 100. The distribution of these events skews toward older populations, meaning that military leadership is likely more affected by serious adverse events or even death associated with the experimental COVID-19 quasi-vaccines.
From 2020 to 2021, the number of ambulatory reports of poisoning by or adverse events associated with viral vaccines leapt from 113 to 1696 in DMED, more than 15 times as high.
Respiratory System (ICD-10 Codes: J00-J99)
Respiratory System (ICD-10 Codes: J00-J99)
While I would have initially focused more on this diagnostic category, it turns out that most of the codes here have no relationship to either COVID-19 or vaccination. A larger portion of serious vaccine adverse events are blood, circulatory, immune-oriented, or related to the nervous system. We will only find interesting elements of the data as we zoom in for a later article.
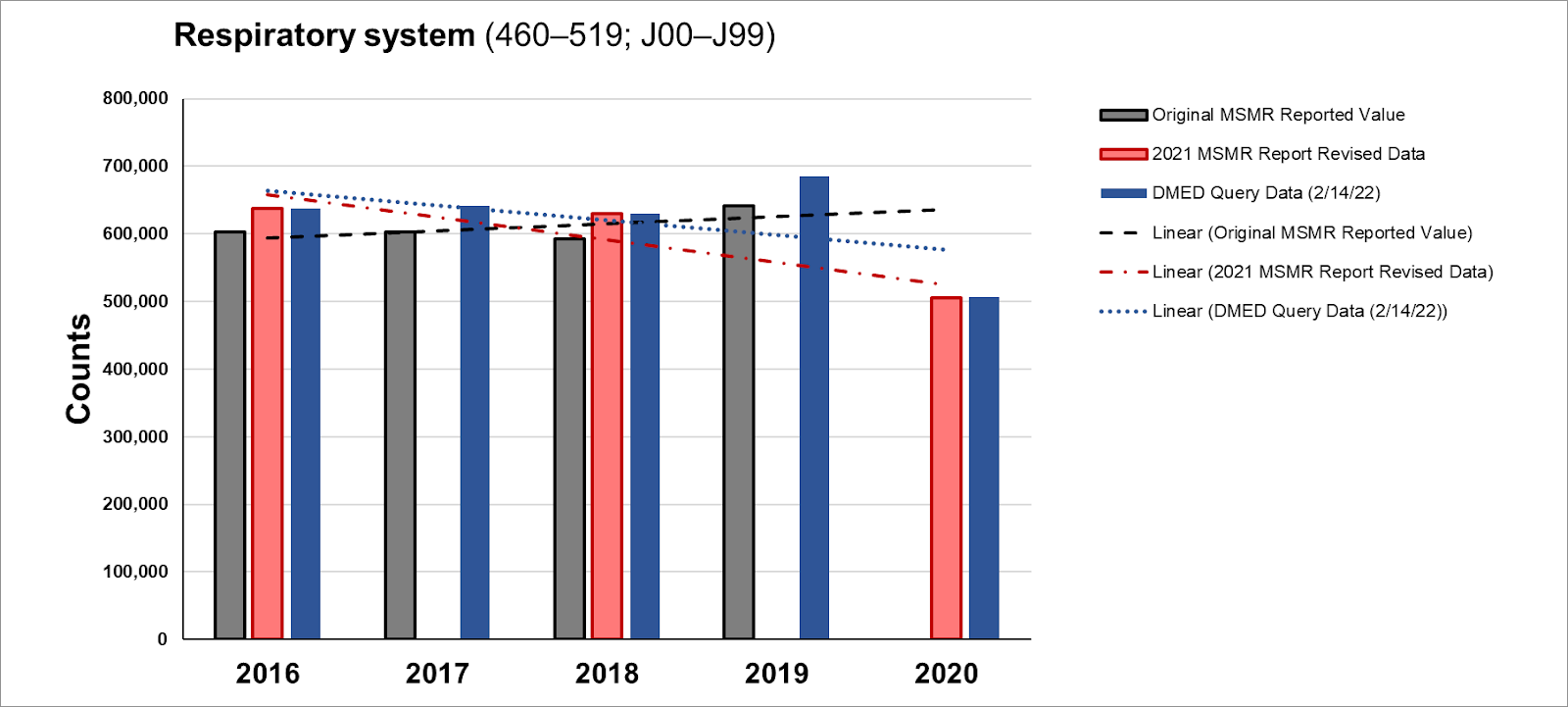
The 2016 and 2018 summary ambulatory data were upwardly revised 6.0% and 6.3%, respectively in this diagnostic category. There are some very serious stories to talk about here, but I'll go ahead and point out that COVID-19 itself was not categorized among the J-codes.
Pregnancy and Delivery (ICD-10 Codes: Relevant Z-codes; O00-O99)
Apologies for not having the DMED queries totals here. I will likely come back and edit this chart later. I was not aware of the missing data when I got started. Basically, I outsourced most of the analysis of this category, so I'll have more to say here when I get into higher resolution stories.
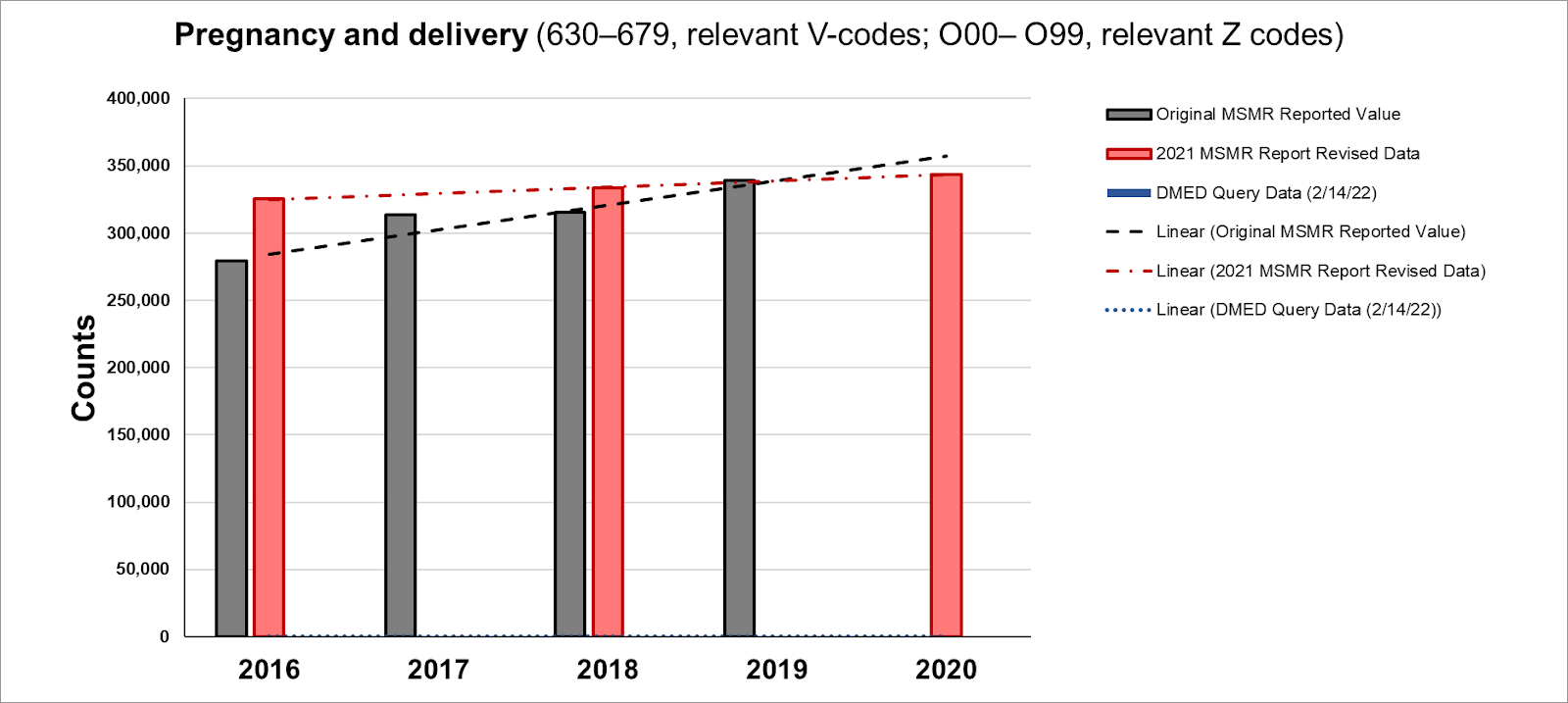
The 2016 and 2018 summary ambulatory data were upwardly revised 4.7% and 5.8%, respectively in this diagnostic category. For obvious reasons, there is a great deal of attention on this category. Even small changes here can have profound effects on civilization. But for the moment we are staying at medium resolution, and I can't drop hints because the workload has been enough (and this category has been toughest to analyze) that I do not yet have answers.
Skin and Subcutaneous Tissue (ICD-10 Codes: L00-L99)
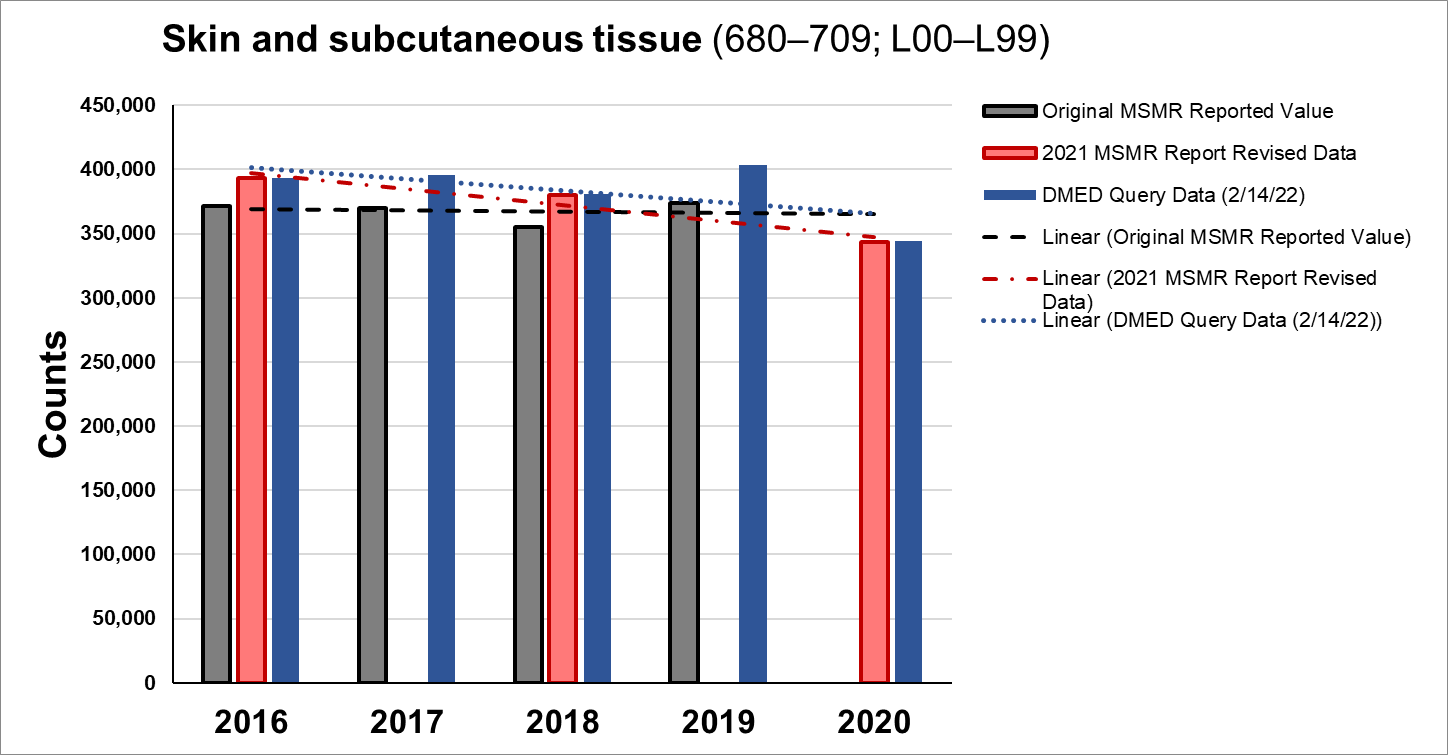
The 2016 and 2018 summary ambulatory data were upwardly revised 6.1% and 7.0%, respectively in this diagnostic category.
Genitourinary System (ICD-10 Codes: N00-N99)
Those worried about fertility issues should look beyond just the pregnancy category. This is one of the categories with related coding for illness and injury.
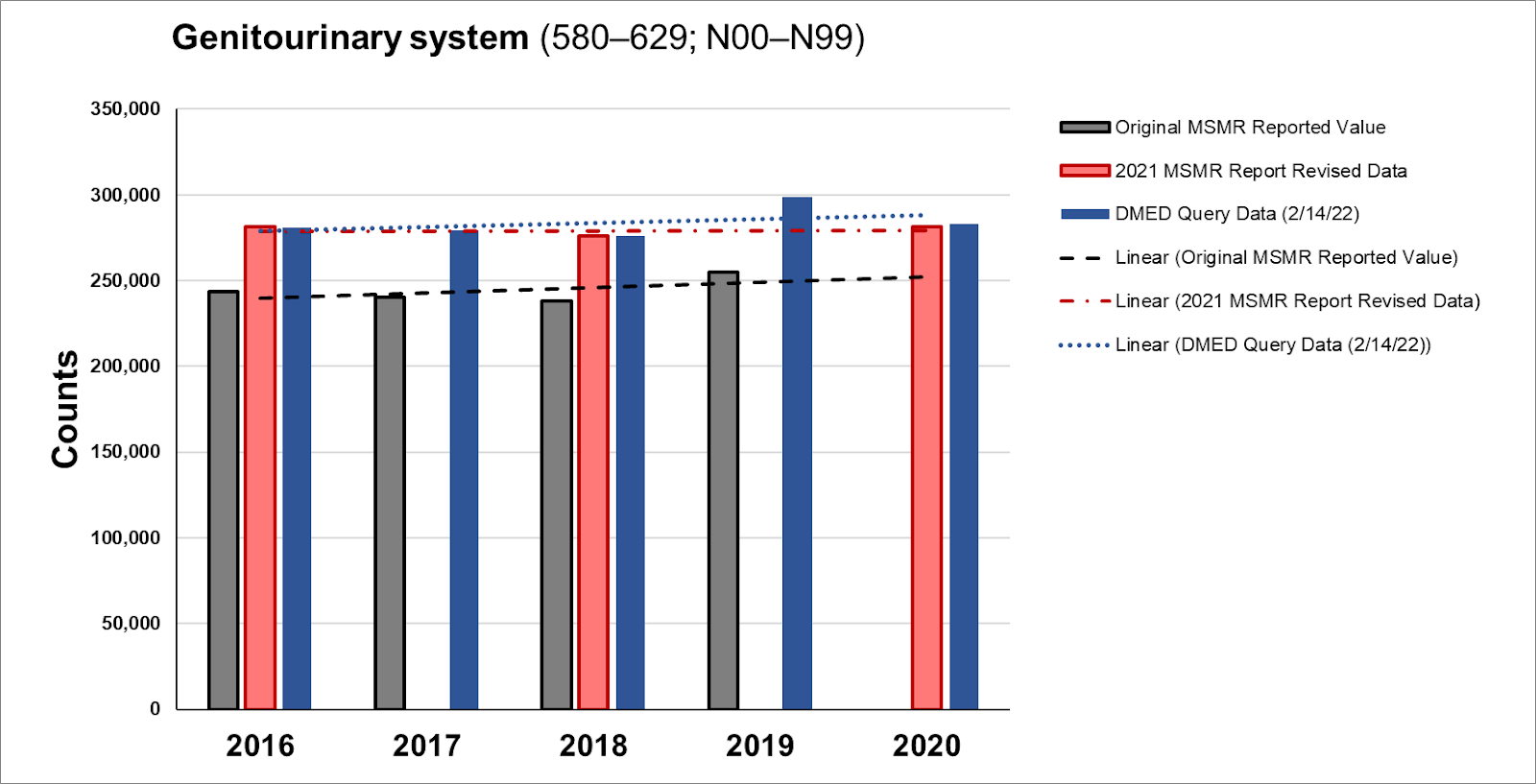
The 2016 and 2018 summary ambulatory data were upwardly revised 15.4% and 15.9%, respectively in this diagnostic category. These are extraordinary changes not to be explained in a database, and the importance of this category of disease and illness cannot be understated since it represents systemic risk to national and world populations.
Digestive System (ICD-10 Codes: K00-K95)
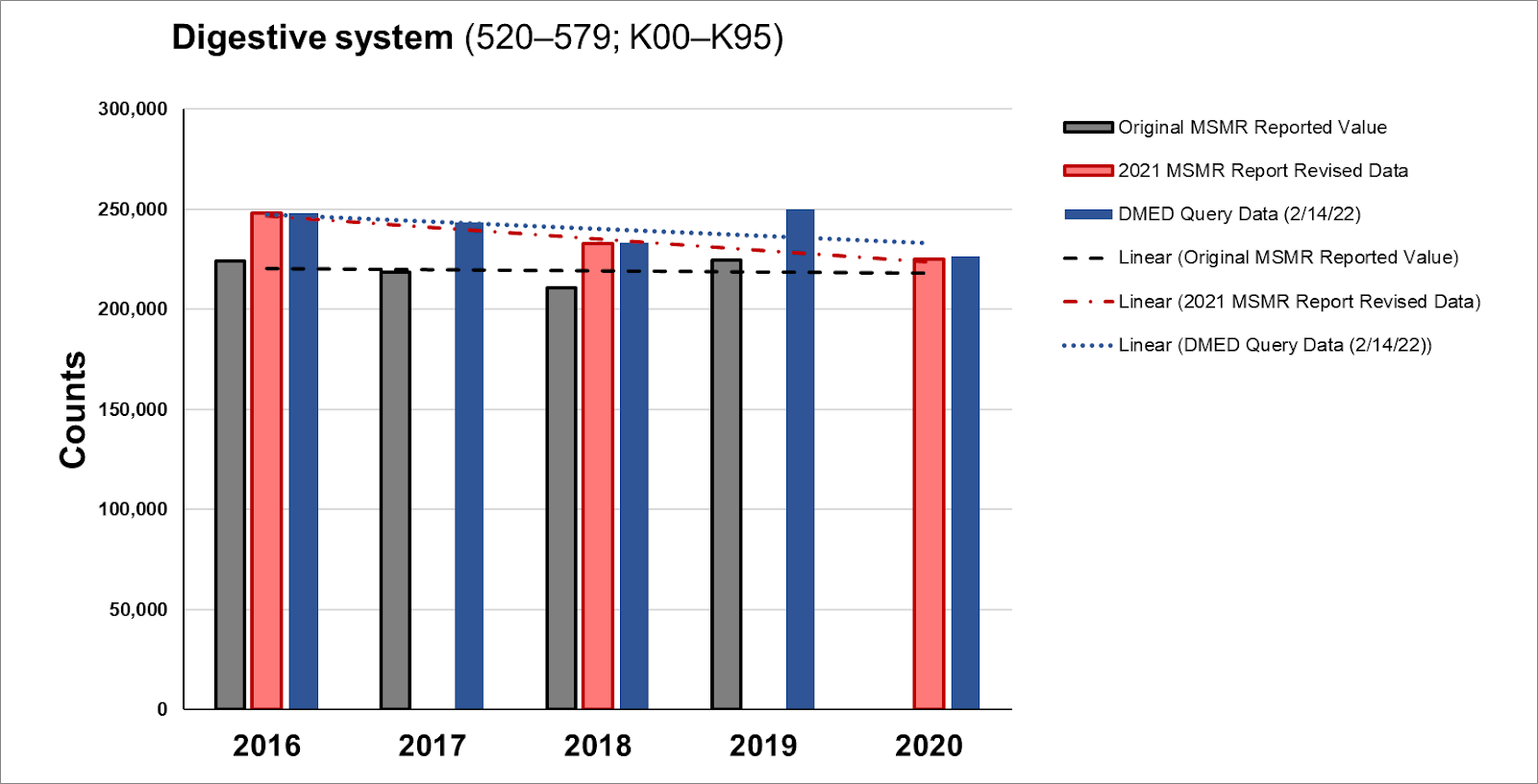
The 2016 and 2018 summary ambulatory data were upwardly revised 10.5% and 10.4%, respectively in this diagnostic category. If a rise in the rate of digestive system illness due to spike protein or some other aspect of the experimental COVID-19 quasi-vaccines is not intuitive to you (and it wasn't at first to me), watch Joshua Guetzkow's talk.
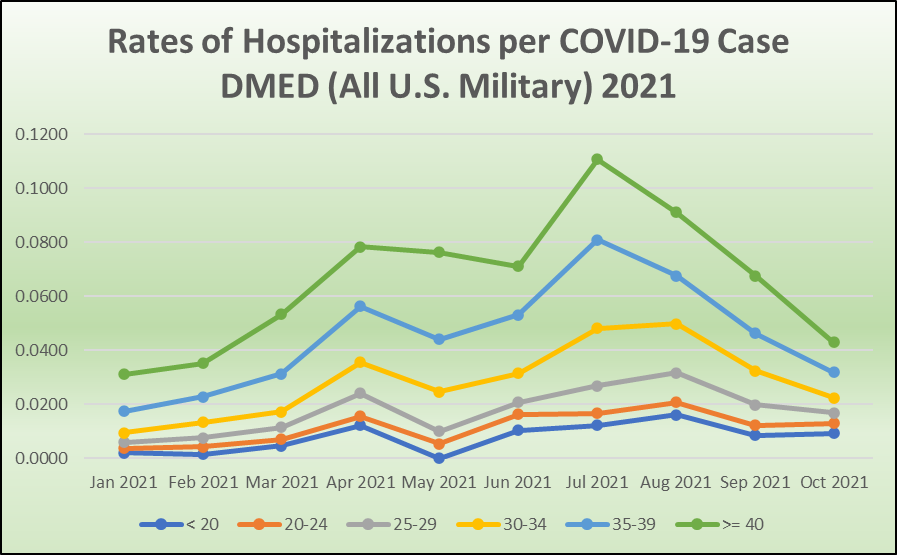
Infectious and Parasitic Diseases (ICD-10 Codes: A00-B99)

The 2016 and 2018 summary ambulatory data were upwardly revised 16.6% and 17.9%, respectively in this highly relevant diagnostic category. There will be a great deal to talk about as we zoom in on these massive upward revisions. But to give a sneak preview, we can see that as the highly vaccinated military moved through their rollout—and especially when the mandates were pushed out in the late summer, COVID-19 cases became more severe on average as indicated by hospitalization rates, among military personnel.
Rates of several key infectious diseases are exploding, and that will be talked about in depth in another article.
Endocrine, Nutrition, Immunity (ICD-10 Codes: E00-E89)
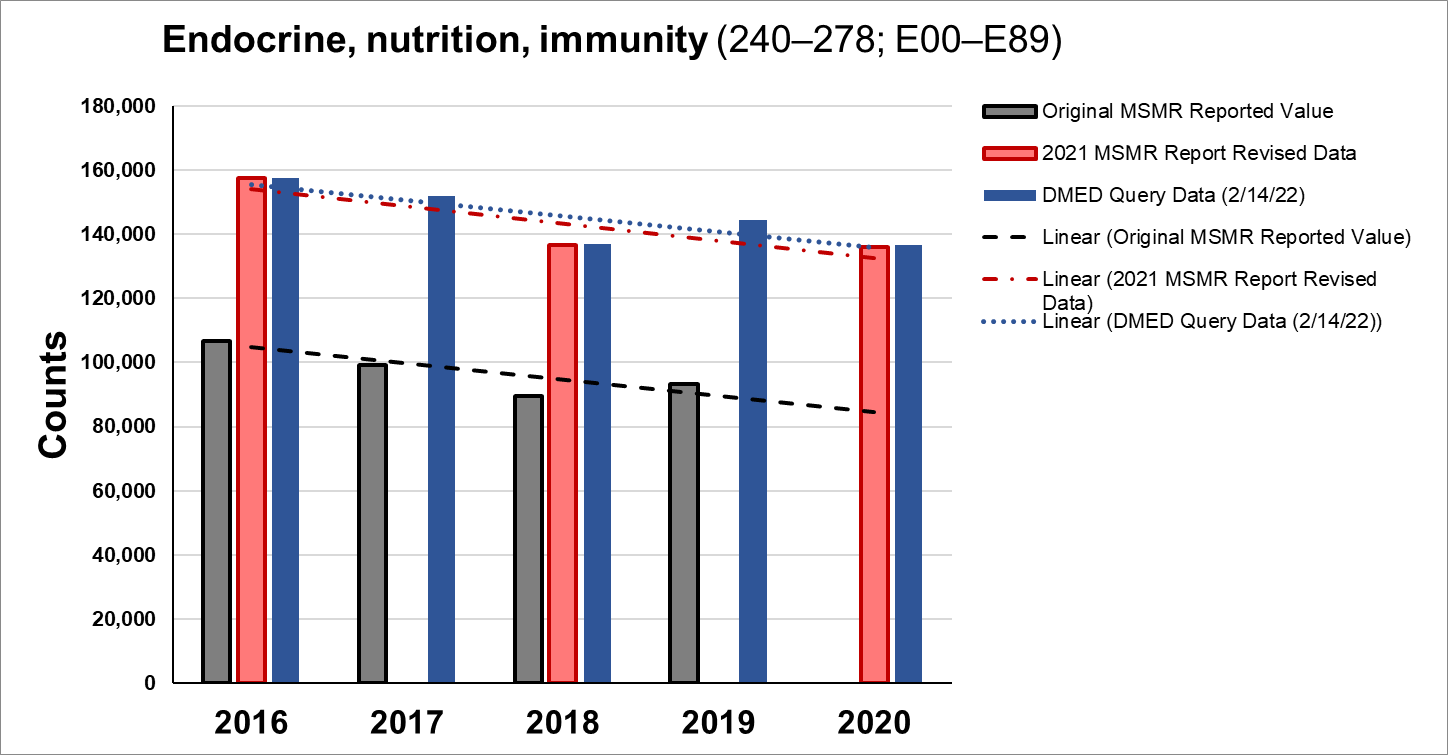
The 2016 and 2018 summary ambulatory data were upwardly revised a whopping 50.3% and 52.5%, respectively in this diagnostic category. We don't even need to drill down to understand the level of hiding massive signals of illness here.
Circulatory System (ICD-10 Codes: I00-I99)

The 2016 and 2018 summary ambulatory data were upwardly revised 13.1% and 13.6%, respectively in this diagnostic category. It will be interesting to drill down to see what safety signals might be hidden by such revisions.
Neoplasms (ICD-10 Codes: C00-D49)
This is the category under which cancers are deposited. The neoplasms are the cancerous growths.
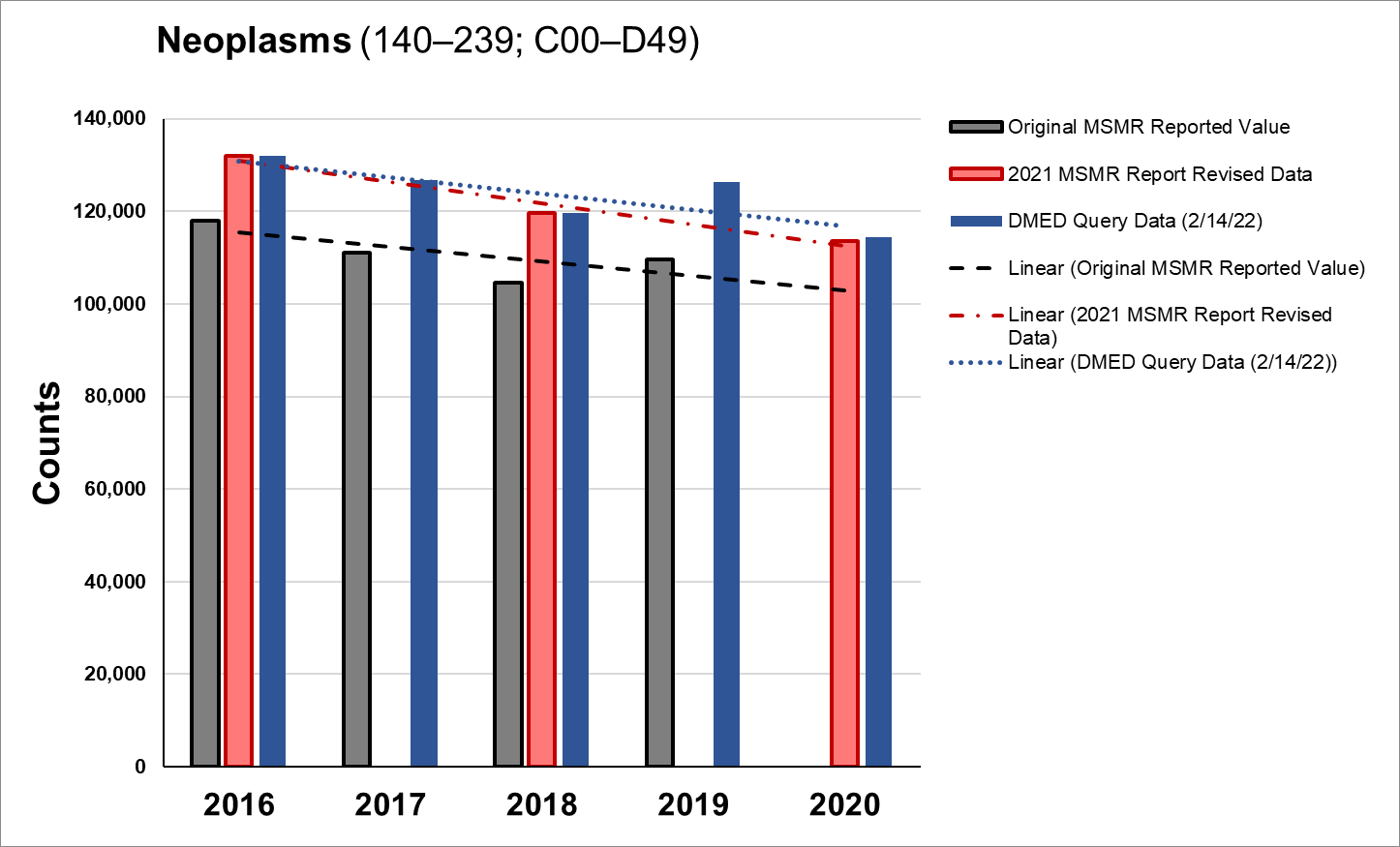
The 2016 and 2018 summary ambulatory data were upwardly revised 12.3% and 14.3%, respectively in this diagnostic category. If these rates were raised to cover up signals from 2021 alone, we're going to see a lot worse, and soon. This is one of the categories I've already explored a bit, but I hope to get a little time asking Dr. Ryan Cole a few questions before I write that article. Dr. Long's stories have been concerning enough.
Hematologic and Immune Disorders (ICD-10 Codes: D50-D89)
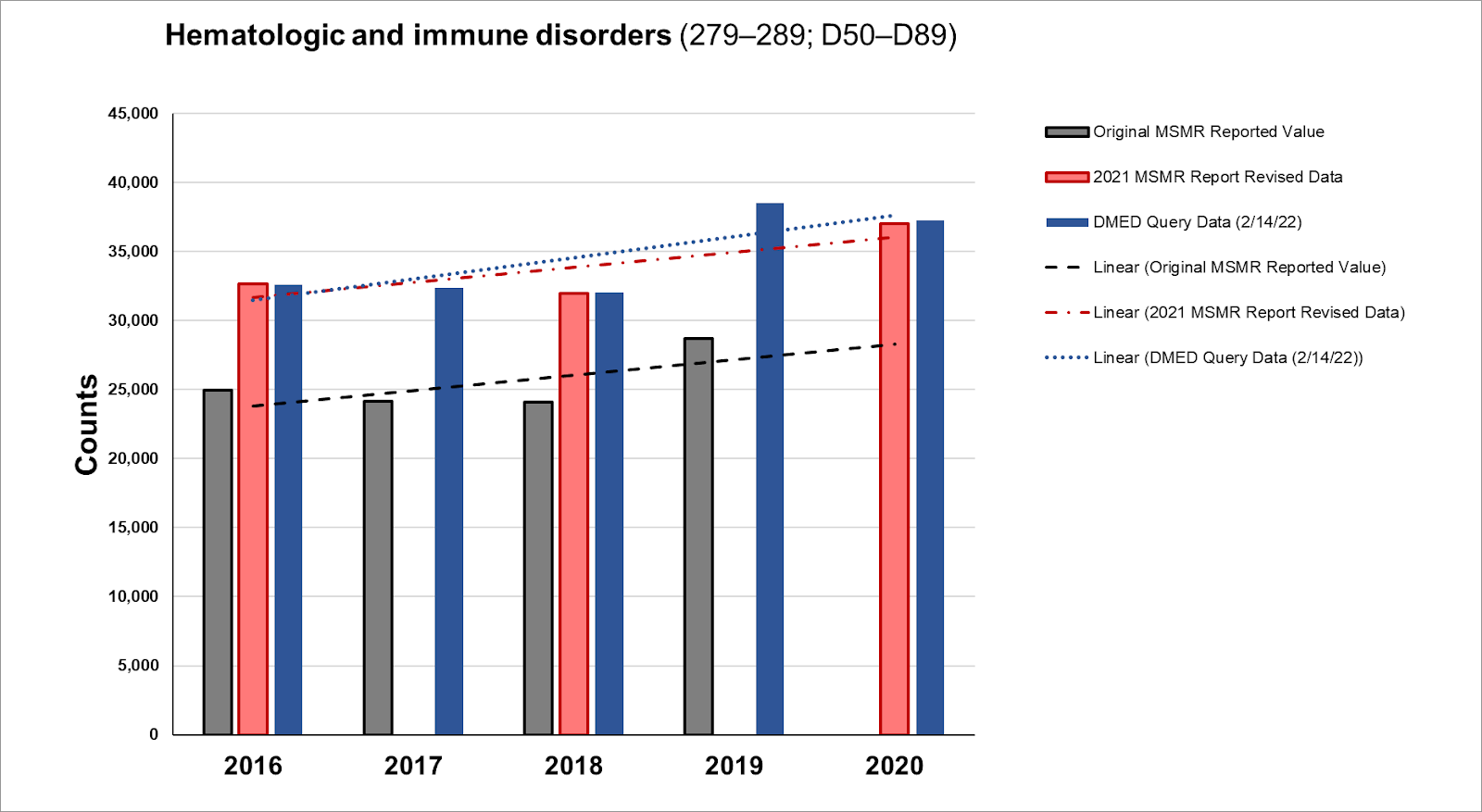
The 2016 and 2018 summary ambulatory data were upwardly revised 31.6% and 32.7%, respectively in this diagnostic category.
Congenital Anomalies (ICD-10 Codes: Q00-Q99)
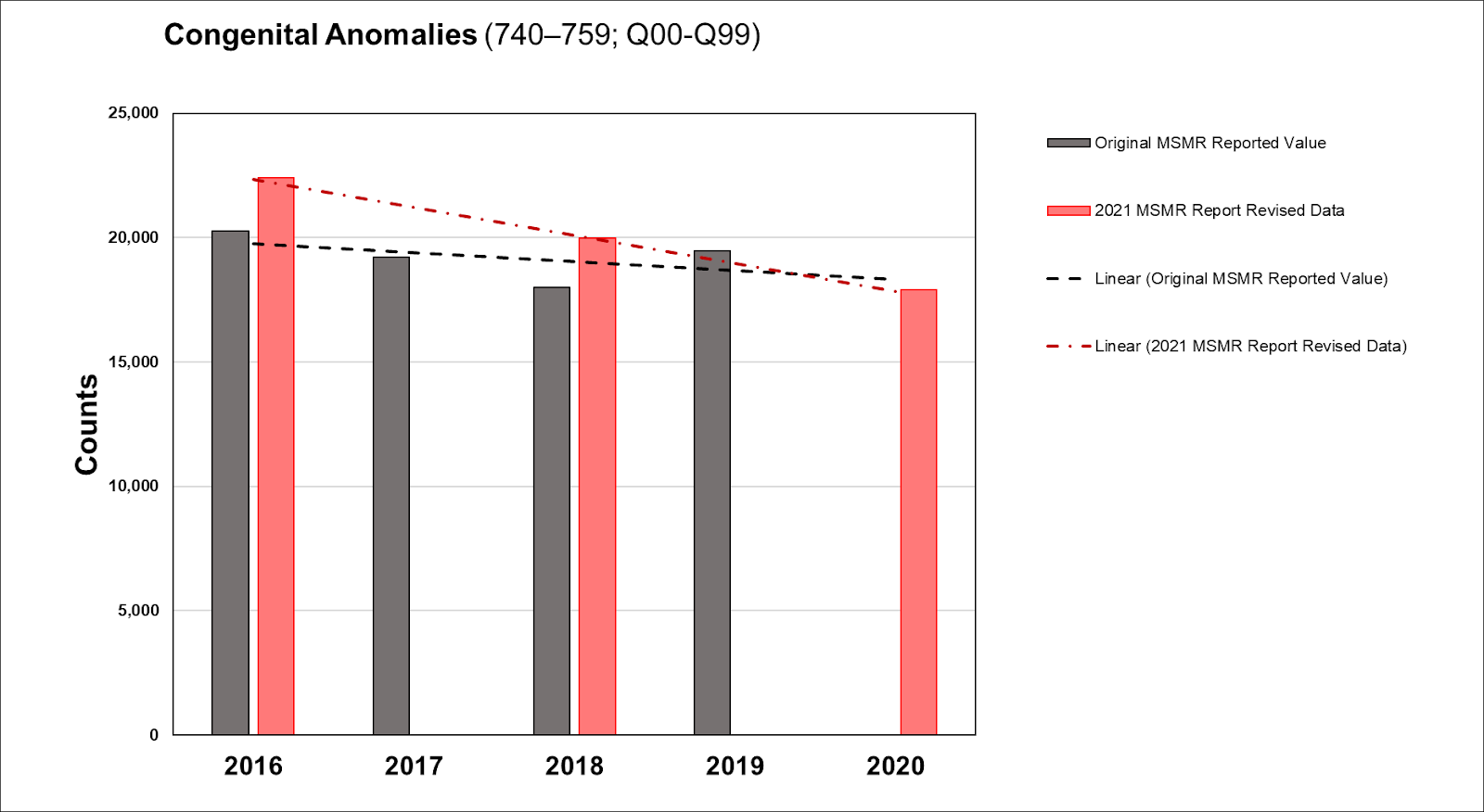
The 2016 and 2018 summary ambulatory data were upwardly revised 9.9% and 11.1%, respectively in this diagnostic category. Unfortunately, I left this category out of initial analysis, so we're piecing this one together now.
Parting Thoughts
If the revisions were not intentionally deceiving, the revelation is that enormous amounts of historical data would have been entirely misunderstood by physicians and biomedical researchers and in crucial ways.
A shout out to the team working with me on this project, which includes not only the three whistleblowers (Drs. Theresa Long, Samuel Sigoloff, and Peter Chambers), but several volunteers who aren't looking for any spotlight and mostly want to remain anonymous. Their courage and humility are felt.
Special thanks to Drs. Heather Gessling, Ryan Cole, Richard Urso, Lynn Fynn, Mary Talley Bowden, and Ben Marble for advice on the next stage of this project that will involve zooming in for higher resolution. In how many ways can these astounding physicians help during all the plandemonium? Whenever I've put in effort with the data, these and others have been happy to step up and spend time with me, whether in framing the context of data, or narrowing my search parameters so that I could work more efficiently. After all, there are hundreds of thousands of ICD-10 codes.
I'd like to once again thank readers and particularly paid subscribers for their support—particularly during this project. It occurs to me that I passed a one year publishing anniversary (has it been that long?), though still not a one year anniversary for the first paid subscription. For the first couple of months, I didn't know there was a button to turn on paid subscriptions. This wasn't intended to be a full time job, but here we are, and I'm grateful to be able to pay the bills having given up my last business plan as I watched such concerning levels of policy and data fraud unfold on so many levels.
It’s all moving at breakneck speed now. 🤯 Thank you for your service.
I’ve believed for a year the goal is total control. If that involves covering up their lies and killing people, they will do it. (Total control gives them those options anyway.)
Dr. Theresa Long, a medical officer with the United States military, has testified in court that she was ordered by a superior to suppress Covid-19 vaccine injuries following the Biden regime’s mandate.
https://dailyexpose.uk/2022/03/25/military-doctor-testifies-ordered-suppress-covid-vaccine-injuries/