


South Africa's Tale of COVID-19, Medicine, and Vaccination
Pandemic National Case Studies

“When you become wise of the healer, also become wise of the sickness.” -South African proverb
South Africa is a nation in long transition on the journey of self-governance since the Apartheid era. Of the large nations of Africa, South Africa has been hit hardest by the pandemic, though its ups and downs tells one of the most revealing stories of COVID-19 pandemonium.
South Africa’s Use of Medicine During the Pandemic
In late march, 2020, South Africa banned the export of hydroxychloroquine (HCQ) in order to ensure its own supply as much of the world looked to the drug as the first line of defense against COVID-19. However, the exact degree to which South Africans have used the drug is hard to ascertain. By policy, South Africa allows that decision to be private between a doctor and patient. Though exact levels of usage of HCQ cannot be ascertained, we know that South Africa was one of the first recipients of HCQ from India after India lifted its own export ban in April, 2020. And we can count South Africa as one of the nations that followed China’s advice of use of the zinc ionophore.
South Africa did sign up for both the WHO’s Solidarity HCQ treatment trial and also a multi-national PrEP trial, the latter of which is ongoing. Some hospitals have reported the choice not to treat COVID-19 patients using HCQ, but do allow independent practitioners working out of those hospitals to make their own decisions.
On August 5, 2020, South African officials published a recommendation against the use of HCQ and some other medications that were surely less available or used. Corticosteroids were recommended in use for patients on supplemental oxygen or on mechanical ventilation. Since that date, COVID-19 fatalities in South Africa have been around 2.25 times as high per day as prior while the worldwide growth rate of COVID-19 mortality has remained very steady. The case fatality rate in South Africa is around twice as high since cessation of its use of HCQ as compared to prior.
South Africa’s Vaccination Campaign
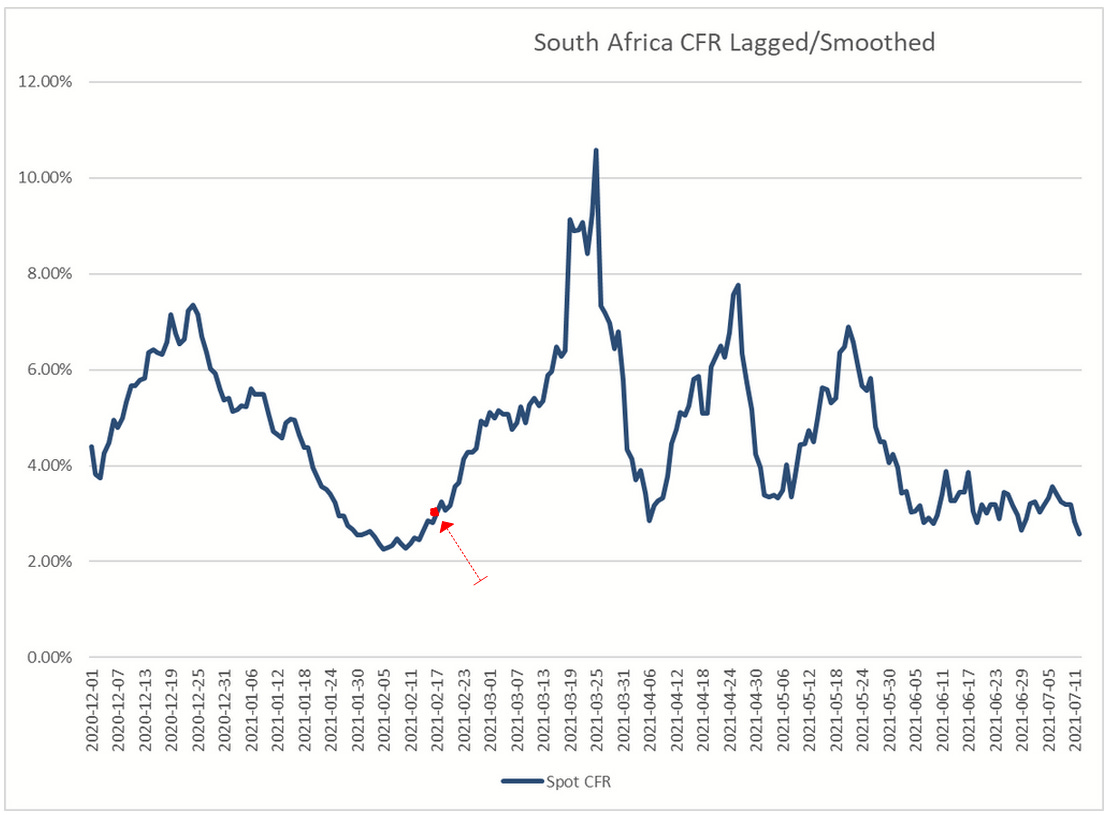
South Africa began its vaccination program at the tail end of its second major SARS-CoV-2 outbreak, on February 17, 2021, employing the Pfizer, CoronaVac, Johnson & Johnson, and AstraZeneca vaccines. South Africa’s CFR, which was 3.00% at the time, jumped to 10.57% over the next 36 days.
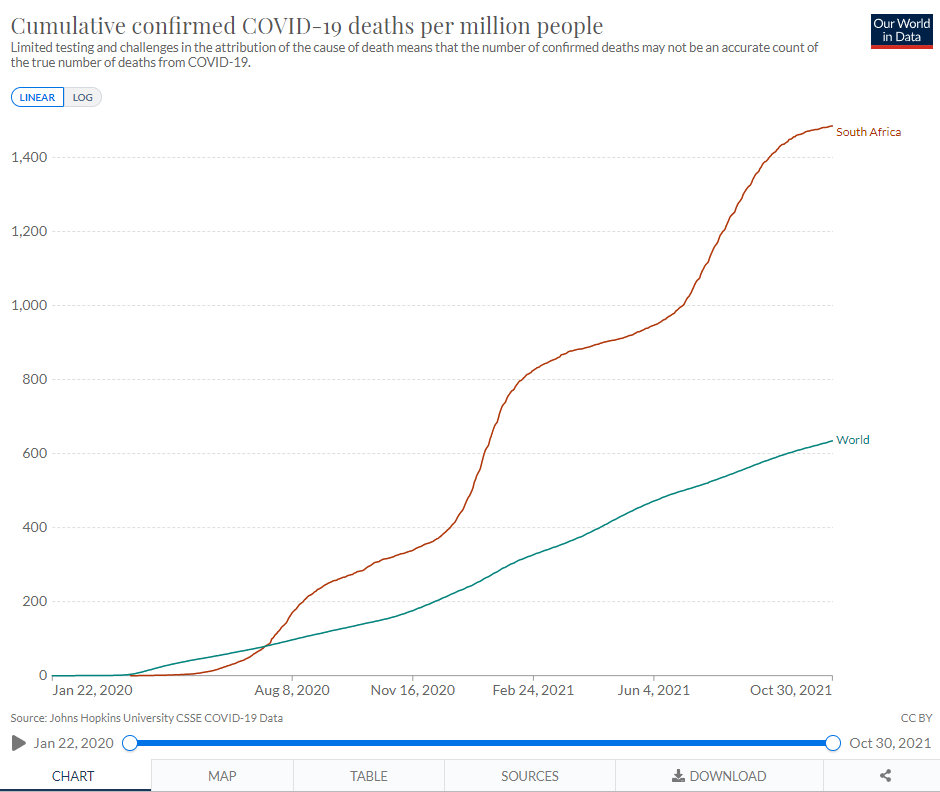
This jump is consistent with rises in CFR while vaccinating elderly populations around Europe. Nearly twice as many South Africans died during its third COVID-19 wave as during its second, which is unusual for a viral outbreak where the second wave is nearly always the highest. It is also inconsistent with the global pattern during the COVID-19 pandemic, as we see in the first chart.
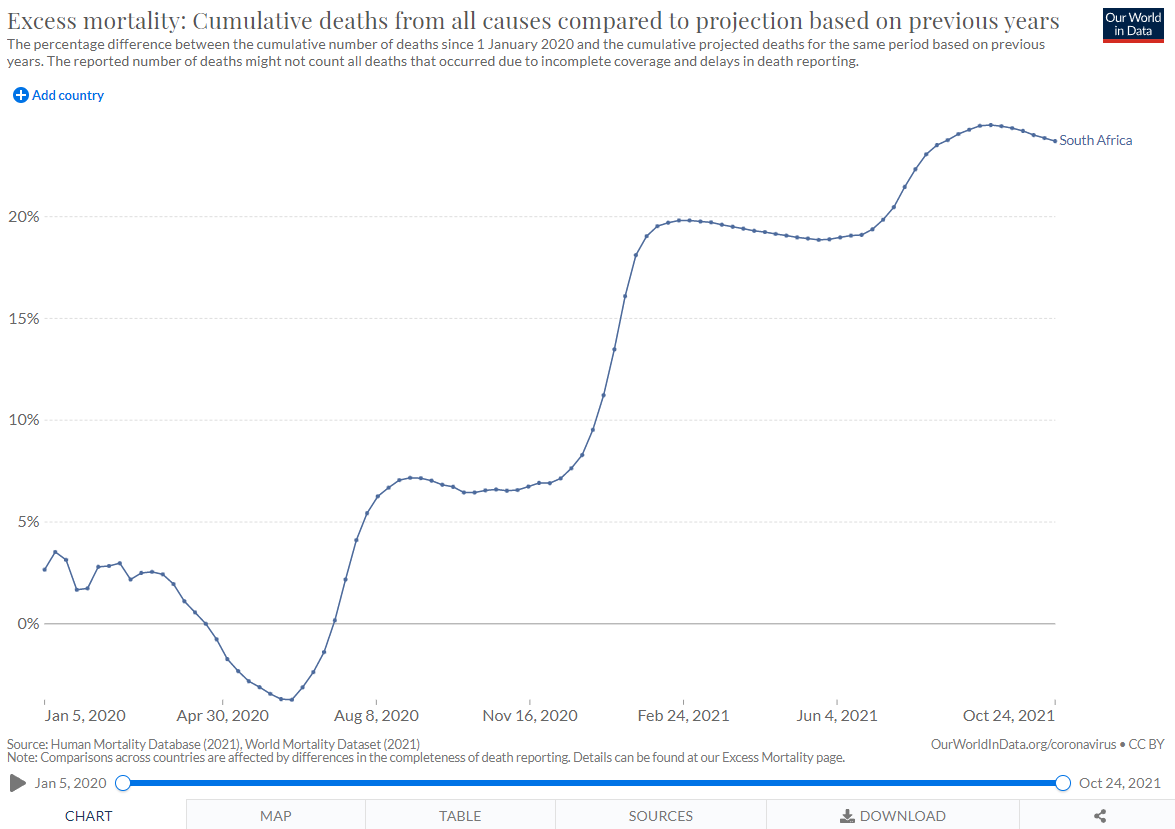
South Africa’s excess mortality trends may shed further light on the efficacy of various interventions. Upon publicly announcing its intentions to secure an HCQ supply, overall excess deaths trended negative, as is often the case following a surge as most surges in excess mortality take place among the most frail who would otherwise make up a substantial portion of those who might have died in upcoming weeks or months. However, excess deaths did not revert particularly sharply after cessation of HCQ usage or upon introduction of vaccines. Each gave way to new waves of mortality.
Corruption among medical officials appears to be a problem in South Africa. On September 29, 2021, the Associated Press reported that former health minister Dr. Zweli Mkhize, who resigned a month earlier in August, steered a $10M “COVID-19 communications” contract to associates who kicked part of the contract back to Mkhize’s family members. This is just a piece of the $900M in suspect contracts in a nation long noted for corruption in the public health sector and provincial health departments (Rispel et al, 2015), that hasn’t found the will to solve the problem. It is enough to make any reasonable person question the purpose of so many billions of dollars in COVID-19 aid to Africa (emphasis theirs):
In Africa, the World Bank’s response is focused around four main areas, simultaneously: saving lives, protecting poor people, protecting and creating jobs, and building back better.
Thanks for all you do Mathew. Are you in contact with @nickhudsonCT/@pandata19 who have a sizeable South African contingent? Mr Hudson is an actuary, I'm sure you know of him.
The Roundtable video from Puerto Rico (?) <https://www.youtube.com/watch?v=4IeVy7jQoz0> has just come to my attention and provides a good opportunity for subscribers to
a) Put a face to your name, and more importantly
b) Circulate the video to friends and family to demonstrate the integrity and passion of early treatment advocates.
Keep going, this body of work is very important.
Am not at all surprised with the banning of HCQ in SA. Are you familiar with Prof. Tim Noakes? http://bitly.ws/iEZv
Even on non-mainstream search engines, a search brings up many articles debunking his current low-carb ideas. Yet prior to his stepping into the low-carb community, due to his development of T2D, his research was highly respected.
Instead rewarding him for identifying the error of his research and reversing his and others' diabetes, the powerful food industry coupled with the medical industrial complex (really, they are the same) went after him.
It always comes down to, follow the money.
Healthcare is a business with an innocent sounding name, that is as ruthless as the tobacco industry, in increasing and maintaining it's market share.
When patients realize that YOU are the product of this corrupt system, you will realize that the system does not care how long you live or how well you live, as long as it gets maximum revenue out of you or your insurance.