


Revisiting Immediate Vaccine Mortality - The CFR Analysis
The Vaccine Wars Part LVII

Bottom Line Up Front: Case Fatality Rate (CFR) analysis points strongly toward vaccine-associated mortality in Europe, and probably also in the U.S., though there is an investigation to perform.
Last year in August when Steve Kirsch and I were still debating whether there was a good way to compute COVID-19 quasi-vaccine mortality to see how underreported VAERS deaths might be, I thought to look at the relationship between vaccination and case fatality rates (CFR) around the world.

If you're not familiar with the CFR statistic, I will explain it down below, and walk through why this analysis deserves more attention. I will also extend the analysis beyond Europe.
The Rationale Behind a Lagged Case Fatality Rate as Indicative of Induced Mortality
The CFR analysis may not be appropriate outside of the West because the West suffered the lion's share of the infection-to-hospital-to-death COVID-19 cases. As I've previously pointed out, there wasn't a whole lot of COVID-19 mortality in other nations around the world prior to vaccination (though it often grew or exploded afterward). Let us define the CFR for COVID-19 as follows:

The basic formula is based on a reasonable, which is to study the severity of illness over time. But there are problems with the way we formulate the statistic, depending on the circumstances:
Deaths lag cases (by a median 18.5 days), so for a local time span, the people are generally mismatched. It is even possible for the ratio to grow above 1, which is nonsensical.
We need a reasonable time span that will smooth out the stochastic noise and weekend biases inherent in such data.
I choose to lag deaths behind cases by 18 days, and to smooth both cases and deaths by replacing the daily new number with the 7-day moving average. Thus, the CFR I use for this analysis is,

This definition for CFR gives us a ratio that would be expected to remain relatively constant over time without differences in demographics, viral characteristics, or medical protocols. For the purpose of this analysis, we hold demographics and viral characteristics constant during the days following the start of vaccination campaigns. While this assumption may not be perfectly true, this author believes the analysis demonstrates a high likelihood of vaccine-induced mortality. Each reader may make their own judgment.
What Happened in the U.S.?
I'm honestly surprised that none of the publishing scientists or statisticians have taken up some version of this analysis. The strongest criticism of it that I've heard is from the anonymous attack dog "The Gift of Fire" (henceforth TGoF), which is that we don't see the same effect in the U.S., but is that really true? Let's take a look.
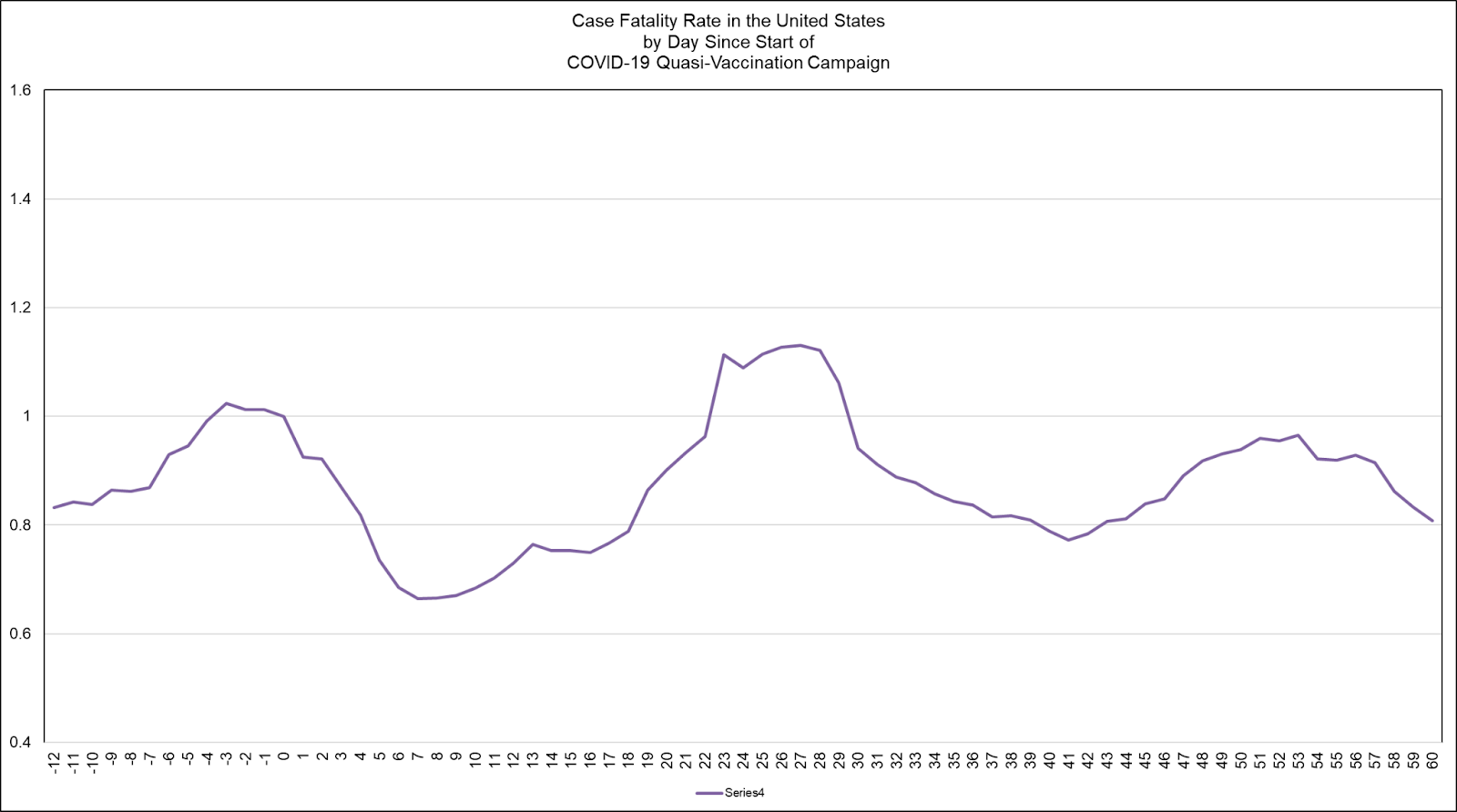
On face, that criticism looks to hold water. At the outset of the experimental, sort-of-tested quasi-vaccination campaign, the CFR quickly drops, but then returns to where it was before continuing onward in what appears like waves of noise. Overall, this already contradicts the claim that the vaccines should make cases less severe. But let us consider whether or not we are working under the same conditions that existed in Europe.
What conditions might affect such an analysis?
How about testing rates?
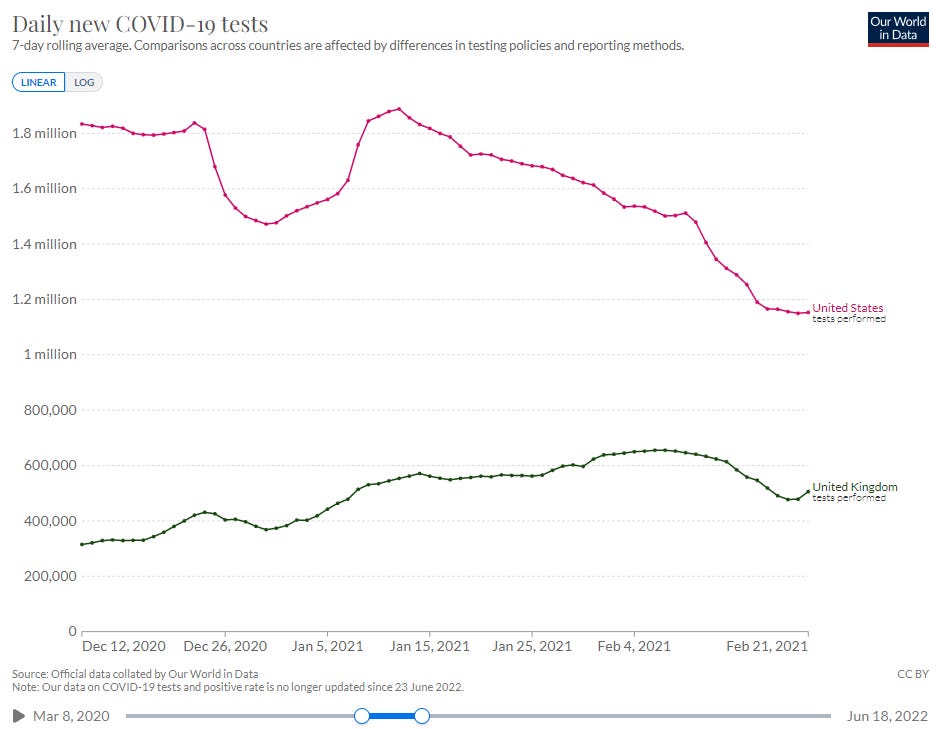
Almost immediately after starting its vaccination program, the U.S. dropped its testing rate, which almost perfectly matches the drop in CFR. As testing came back, so too did the CFR grow back. Then the U.S. began to taper off the testing program substantially. So, what happened?
Let's zoom in on the appropriate parts of the U.S. testing and CFR curves…
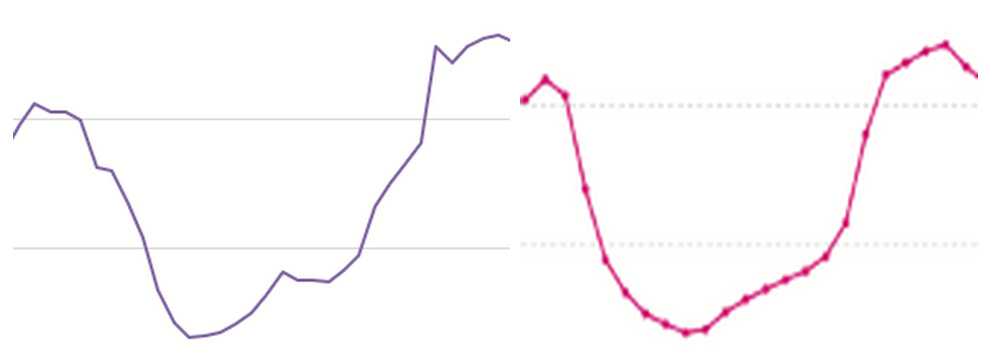
Holy testing shenanigans. To the BatCoV!
Note that TGoF's primary reason why CFR might move around is testing. We agree on that point, but why then did he not make the obvious observation about the same of the CFR and testing curves?
So, what changed about the testing program?
I don't know, but we should find out!
One possibility is that U.S. public health was already aware of the mortality spike associated with the UK quasi-vaccine rollout and decided to hide the problem.
If I were in charge of hiding the problem, I would tell medical examiners to stop testing dead bodies or people coming into the ER injured for COVID-19 because, "Vaccines are here! So it's not going to be a problem," which is basically the way Public Health officials sold the program.
Recall what we have learned about public health officials directing medical examiners in the inclusion of COVID-19 on death certificates when positive testing had nothing to do with the fatality.

It is not much of a stretch to suggest that posthumous testing was halted for roughly a month, or that the inclusion of COVID-19 on death certificates was halted for roughly a month.
TGoF goes on to examine the hospitalized CFR in Europe, but this introduces new variables. He also doesn't cite any data source. He further suggests that Kirsch and I are grifters, which is a weird claim to make about two guys who each likely gave up in the upper-90 percentages of earning potential in order to work out what's going on. All criticism is fine, in a sense, but criticizing people who make good livings from their analytical skills (in highly competitive domains) while hiding behind the veil of anonymity seems…cheap.
TGoF also suggests that I must be seeking status, which is probably the reason I've seven times turned down offers to take the helm of various hedge funds (one of those invitations came from Steve last year). Of course, anons can sling mud and remain anonymous, shielding us from discovering their own interests. I did make my usual invitation to TGoF to come to the table in a recorded conversation. No answer.
Back to testing policy deviation…If you're thinking that a testing policy deviation would affect both the numerator and denominator of the CFR fraction, you're right, but the point of a targeted policy is to affect the CFR in the most pronounced way, then continuing to test at schools, among air travelers (which were many during the holidays), and drive-in boxes while stopping testing among those dying is the best way to achieve the desired result. After that, all that needs to be done to pull the CFR downward (to create the appearance of vaccine efficacy) is for people in nursing homes to stop dying so much…check!

Afterthoughts
Last year when I was flooded out of my home, I had the spreadsheet for this analysis open. I did not realize at first that I'd lost a lot of work on it, but I did. Being homeless for three weeks, then catching up after getting into a home pushed this additional analysis, which would have been completed in November, forward a bit. Then came the book. Then came the DMED analysis which has drained perhaps 800 hours from my life. In all that time, a good analyst could have repeated the analysis for checking in a day or two. The U.S. piece took additional thinking, but I have always been happy to talk it through.
We have a serious lack of stats minds caring to work on these problems. This is concerning. We will not achieve a world of great freedom and prosperity without people taking responsibility for sorting out challenging problems during challenging times.
Mathew, I deeply appreciate your time, money, effort, sacrifice here and ongoing for humanity. That's probably no consolation to what you have sacrificed. As much as trusting the science, RCTs etc, that one would have believed in 1 year ago, it's nice to have someone like you who hasn't been corrupted (or so it seems😉). I recognize there are multiple explanations for what the data flushes out and our leaders wouldn't want to think that hard. It might collapse the house of cards. Have you been following Coque de.Chien and his case in Massachusetts for falsifying death certificates. I feel like there needs to be a war room where a group of you locks yourselves in the room and hash out theories and possibilities. If you do that, I would love to see that live from a zoom link. It would be fascinating to listen to a group of thinkers! I may not understand it all, but I am sure the energy in the room would be something to witness. Again, thanks for carrying on!!!
This is why I will continue to pay for this 'stack in perpetuity.