


My Dangerous Talk at a City Council Meeting
The Chloroquine Wars Part LXXX

"As soon as there is life there is danger." -Ralph Waldo Emerson
This past Monday, Honolulu City Council Floor Leader Andri Tupola contacted me and asked me if I could address the city council with information and statistics about early treatment options for COVID-19. Such a talk would further support the early treatment kit program established by the firefighters, but also serve broad educational purposes. While I have several research projects on my high priority list, and scores of articles to work on, community outreach is one of the few things I'm willing to drop everything to support. I've often said, "Community is the most underrated technology," which is more than just a warm and fuzzy slogan (really, click the link).

I was encouraged to stay away from words like "ivermectin" and "hydroxychloroquine" due to the strange and psychotic cognitive dissonance surrounding them. "Okay," I thought, "I can do that."

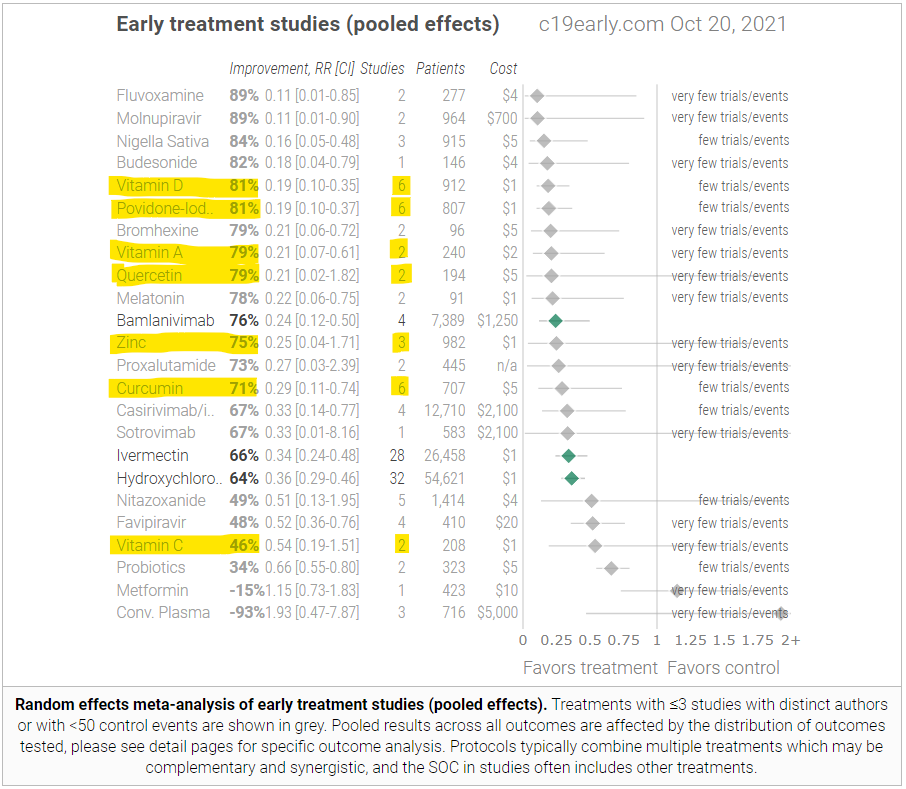
My goal would be to can a friendly, but powerful talk, with heavy citation, that would hopefully help anyone willing to maintain an open mind that we are missing the mark entirely regarding vitamins, minerals, and zinc ionophores (which include chloroquine and hydroxychloroquine, but also quinine, quercetin, ECGC, curcumin/turmeric, and many more), not to mention simple hygienic solutions such as keeping windows open and cleaning the mouth, nose, and throat to prevent infection. In a subscribers only post, I will post the entirety of the talk I gave, which I plan to refine for future engagements (perfection of a 10 minute talk cannot happen in 30 hours with full citations). There were gaps in information such as all measurements of vitamin deficiency and hazard ratios in published research to date.
Tuesday I attended the council meeting by zoom. There was various city council business after which Dr. Robert Malone, Dr. Robin Armstrong, and myself gave various 10ish minute presentations and took questions from city council members.
I was amused and a bit surprised when, after my talk, Chairman Tommy Waters immediately declared my testimony "dangerous and irresponsible", though two members of the council defended my presentation.
Behold, The Science!
The news coverage of the meeting is both humorous and sad. You really should watch the video on that link to soak up just how captured the media outlets are.
“I actually think what this person is testifying to is actually dangerous and irresponsible,” said Waters.
The mainland speakers include Mark Crawford, the statistician, Dr. Robert Malone of Virginia, who has been critical of the vaccine’s effectiveness, and Dr. Robin Armstrong, of Texas, who advocates the use of monoclonal antibodies.
“I just want to make clear that what this person is testifying to ― and for that matter Dr. Armstrong or even Dr. Malone ― is not something the Council as a body is endorsing, is supporting or is in any way legitimizing.”
I'm not sure who this "Mark Crawford" fellow is, but I have to wonder if somebody in the newsroom was worried that viewers might find my dangerous substack. More amazing is the suppression of Dr. Malone's credentials as the inventor of mRNA vaccine technology. I honestly felt that Dr. Malone pulled most of his punches---possibly at least partially for reasons of diplomacy engaging an audience with hostile members. I mean...if sharing information about vitamin deficiency and supplementation with respect to the current pandemic is "dangerous and irresponsible", I can't imagine how, "This vaccine is broken and the spike protein seems to breach the blood-brain barrier" might be received.
Mathew Danger Crawford -- Danger is My Middle Name
Now that I'm the "dangerous vitamin-promoting statistician", I'll need to revise my image. I've never owned a motorcycle, but I've maybe got the facial hair to sell an image with a Harley and a leather jacket? I'm sure the Hells Angels will understand who is alpha when they see my Zinc Ionophore Statistician logo (currently under development). I'm taking advice from Dr. Rollergator, PhD on the matter.

1/2 Hi Mathew, Vitamin D is by far the most important early treatment for COVID-19. In the longer term we must boost most people's circulating 25-hydroxyvitamin D (as measured in blood tests) to 50ng/ml (125nmol/L) or more, since levels lower than this cause weakened innate and adaptive immune responses, and increase the risk of hyper-inflammatory dysregulated immune responses which drive severe COVID-19, sepsis, Kawasaki disease and Multisystem Inflammatory Syndrome. Typical unsupplemented levels are 5 to 25ng/ml.
Most people cannot imagine that lack of vitamin D3 - sitting on supermarket shelves - is the decisive factor which causes such disease severity and so viral shedding that we have an R0 well over 1.0 and so a pandemic with millions of deaths. This includes especially most physicians and immunologists - but they should read the research. Long ago they should have heeded the 2008 call by 48 physicians and researchers (some are both) for 40 to 60ng/ml to be regarded as a proper, healthy, 25-hydroxyvitamin D level: https://www.grassrootshealth.net/project/our-scientists/ .
There is very little vitamin D in food or multivitamins. UV-B exposure of unprotected skin (not through glass or sunscreen) can produce plenty of vitamin D3, but this is not available all year round, raises the risk of skin cancer, and is less effective for those with dark skin. Without proper D3 supplementation or recent significant UV-B exposure, most people's 25-hydroxyvitamin D levels are between 5 and 25ng/ml - 1/10th to 1/2 of what their immune system needs to function properly.
Most doctors accept outdated official recommendations that 20 or perhaps 30ng/ml is sufficient, and some still think that for an average weight adult, 0.01mg (400IU) D3 a day is sufficient to meet a person's needs. For 70kg 154lb bodyweight, 0.125mg 5000IU D3 a day will get most people's 25-hydroxyvitamin D levels safely to 50ng/ml or more after several months. This is a gram every 22 years. Pharma grade D3 costs USD$2.50 a gram ex-factory, in 1kg lots. There are only a handful of D3 factories in the world, none of them owned by multinational pharmaceutical companies. Most D3 is made (for a lower price, with less refining) for poultry and pigs who live their lives indoors. If the big pharmaceutical companies could devise and patent a compound even a fraction as effective as D3, they would sell it for hundreds or thousands of dollars per monthly dosage.
D3 is hydroxylated in the liver over a period of days into 25-hydroxyvitamin D, which goes into circulation and diffuses into all tissues. This is what all immune cells need for their autocrine (inside the cell) and paracrine (to nearby cells) signaling systems, which are crucial to each cell's ability to respond to its changing circumstances. These systems are activated by particular conditions (different for each cell type) and hydroxylate 25-hydroxyvitamin D a second time to become 1,25-dihydroxyvitamin D, which strongly activates vitamin D receptor molecules in these cells. The activated receptor turns up the transcription of dozens of genes, and turns it down for dozens of other genes, in ways which are specific to each type of cell. These signaling systems are long-evolved, flexible, powerful, methods by which cells change their behaviour according to particular conditions they detect.
Vitamin D based autocrine and paracrine signaling has nothing to do with the one hormonal function of the vitamin D compounds - a very low level of circulating 1,25-hydroxyvitamin D, produced and regulated by the kidneys, as part of a larger feedback loop with the parathyroid hormone, to regulate calcium and bone metabolism. All doctors know of this system, and most have some idea that the immune system needs vitamin D. However, very few understand - of have heard of - vitamin D based autocrine and paracrine signaling, in part because the vitamin D researchers have not explained it well. Please see my explanation, which cites the original research over ten years ago by Martin Hewison et al.: https://vitamindstopscovid.info/02-autocrine/ .
Here are the most important research articles from those cited at "What every MD, immunologist, virologist and epidemiologist should know about vitamin D and the immune system": https://vitamindstopscovid.info/05-mds/ . Please read the research yourself. Don't take my word for anything - I am an electronic technician and computer programmer.
In 2014, researchers in Boston MA, (Quraishi et al. link and graph at https://vitamindstopscovid.info/05-mds/#fig01) analysed the relationship between pre-operative 25-hydroxyvitmin D levels and post-operative infections: surgery site infections and general hospital-acquired infections. The relationships were similar: with 25-hydroxyvitamin D levels of 50ng/ml or more: 2.5%. With 18ng/ml - which is a typical average value for people who do not supplement D3 or get much UV-B skin exposure - the risks for both types of infection rose to 25%. This can only be explained by weakened innate and adaptive immune responses to bacterial pathogens caused by insufficient 25-hydroxyvitamin D.
Low 25-hydroxyvitamin D levels cause the same weaknesses in innate and adaptive immune responses to viruses, including SARS-CoV-2. See the risks of severe COVID-19 according to Venegas-Cedillo et al 2021 and 3 other studies, plus the risks of Kawasaki disease (2014) graphed as a function of 25-hydroxyvitamin D levels: https://vitamindstopscovid.info/05-mds/#fig02 . Most doctors and all governments have been clueless about this. With the exception of a few doctors and governments (such as of the Indian state of Uttar Pradesh, who use ivermectin with great success) people have not been supported with vitamin D and other nutrients and have been prevented from getting early treatment of any kind. They were told to get vaccinated, isolate if infected, and to seek hospital treatment if hypoxia sets in. Very few of these millions of people needed to die. Vitamin D and other early treatments would have prevented most of the transmission, harm and death.
The sooner these graphs and links the articles are plastered all over newspapers and MSM websites, the better. Then everyone will know the truth. This is not the pandemic of the unvaccinated. It is the pandemic of the vitamin D deficient and of those who have not been able to receive early treatment.
I find this ignoring and stifling of early treatments and prevention supplements the hardest proof of sinister motives.