

Did RTE's Investigation Force the DoD to Stop Publishing the Military's Health Data?
Did RTE's Investigation Force the DoD to Stop Publishing the Military's Health Data?
The Wars of the DoD, Part 3

"Facts are stubborn things; and whatever may be our wishes, our inclinations, or the dictates of our passion, they cannot alter the state of facts and evidence." -John Adams
It very much looks that way.
Here is a link to previous articles about the Department of Defense's (DoD's) medical databases and the controversy around "updated" data viewed in the DoD's database snapshots.
Over at Health.mil (scroll down), the May 2022 Medical Surveillance Monthly Report (MSMR) finally appeared, but without the usual snapshots of either the ambulatory or hospitalization data (the ambulatory data is where manipulation seemed to occur). The indexes of the 2021 May MSMR on the left and the 2022 May MSMR on the right for comparison:
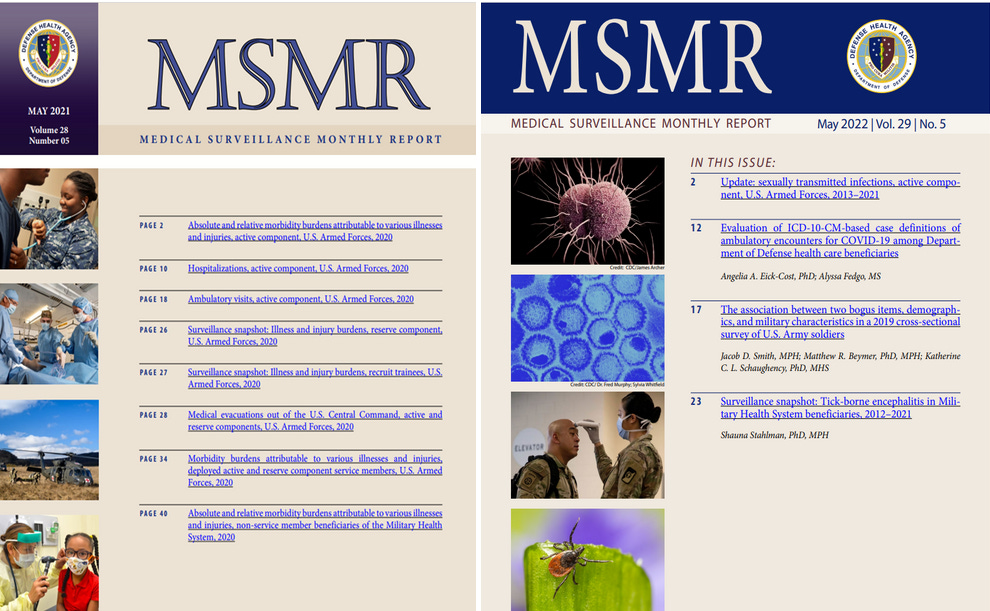
Here are side-by-side views of the index of the last two May MSMRs. The current edition…looks kind of bare, don't you think? Like they did not plan more articles because the second and third articles are expected to contain all those graphs and charts that we usually see? Having looked through a few dozen MSMRs from prior years, I think this is the shortest edition to date.
Huh.
Why would the DoD stop publishing snapshots of the DMSS/DMED data?
Recall that I identified not one, but two manipulations of the data. The first was applied to all major ICD-10 diagnostic codes that likely took place just prior to the 2021 MSMR. We see the result of this manipulation visibly.

Then came the August 2021 server migration. But after that, somebody felt the need to make major alterations to just the R-code data. This became apparent after the DoD fixed the glitch introduced during the server migration (remember, I do believe they fixed some problem pulling in 2016-2020 data at the end of January, regardless of the nature of the glitch). Consider the graph below of just the R-codes:
Manipulation 1: Grey to Red.
Manipulation 2: Red to Blue.
The problem for the DoD is that this second chance, which is dramatic (46.6% increase; the two together nearly 60%) is that these newer totals (shown below) would once again bump up the above graphs in the May 2022 MSMR!

The May 2022 MSMR was either going to provide further demonstration of the second manipulation, or the DoD was going to have to stop publishing the database snapshots.
They chose to stop publishing.
Can there be any doubt that these manipulations are meant to hide the grave damage being done? (Can there be any doubt that there are people at the DoD reading Rounding the Earth?)
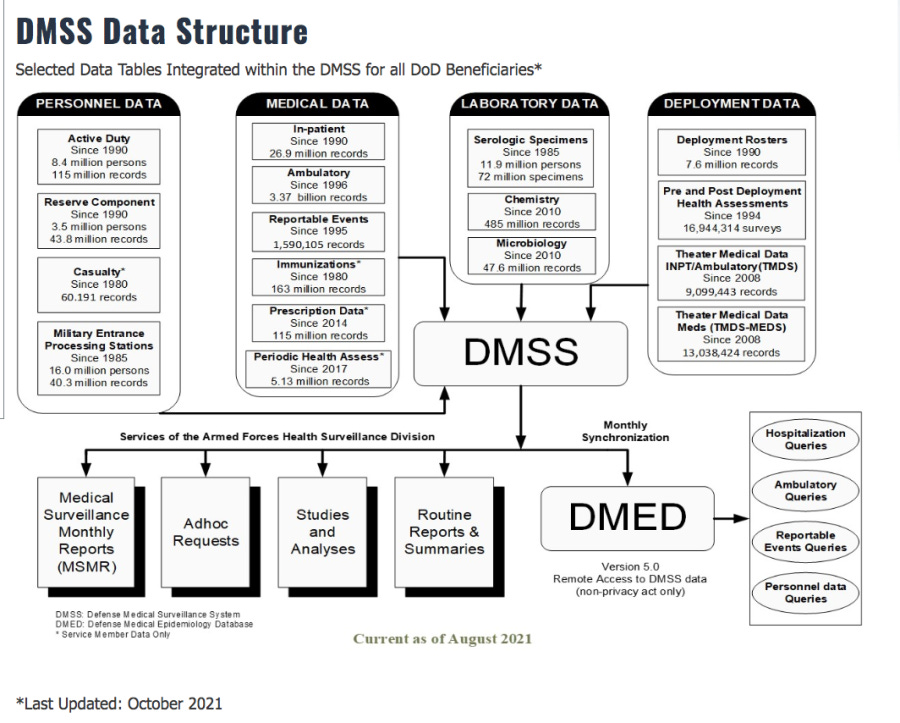
Now, let's go back to the glitch and the server migration. As Daniel Horowitz reported, the claim about the glitch was that there was a problem with the refreshing during the monthly sync between the DMSS and DMED.

This is consistent with problems that might occur if the DMSS data was re-indexed. In other words, if new data was added out of order, with sequential record keeping, then fabricated records would be obviously far away from the genuine data from 2016-2020. Re-indexing would be necessary to hide this problem from anyone investigating the database—just create a new sequence of numbers to identify all records and associate them directly with dates of reporting (including fabricated dates). The monthly cron job was likely insufficiently programmed to handle the re-indexing.
Will All the Facts Be Revealed?
Just this year, the U.S. military announced that they're migrating to new health data systems. What…interesting timing.
https://health.mil/News/Articles/2022/04/08/MHS-GENESIS-Now-Deployed-at-66-of-138-MTF-Commands

Note below that the August date of the new medical data structure matches the time frame of the server migration.
The split rollout of the Military Health System Genesis (MHS Genesis) will splinter the nature of the health data in a way that makes apples to apples comparisons of the health data difficult if not impossible.
With so many facts and so much detail pointing toward my assessment of what happened with the DMED, you would think this story would be front page news—at least among the new media of what might be called the Rebel Alliance. We may not have another chance to unravel everything going on with military health, which stands out as an excellent population (most of the 1.3 million active duty members fall into similar age/profile demographic bands) for study.
I'm also going to share this chilling fact with you: While a handful of people have stepped up to interview me about the DMED story, almost two-thirds of those interviews have never been released. Each of those unpublished interviews has been sitting on the shelf for one to three months. That's in addition to the fact that numerous people who requested interviews ghosted me. This includes interviews with several media names of substantial weight.
Remember: There is an ungodly amount of money in all this. It's being sloshed around everywhere. If you have a favorite media icon, ask them if they know about this story, and do not let them act like it stopped at the Johnson hearing and glitch claim.
Military Mortality Data
Also recently released—months after we would usually see it—is the 2021 summary mortality data from the U.S. Armed Forces. I'll leave it to you to decide whether or not we can trust the data. One way or another, we can make some interesting observations.
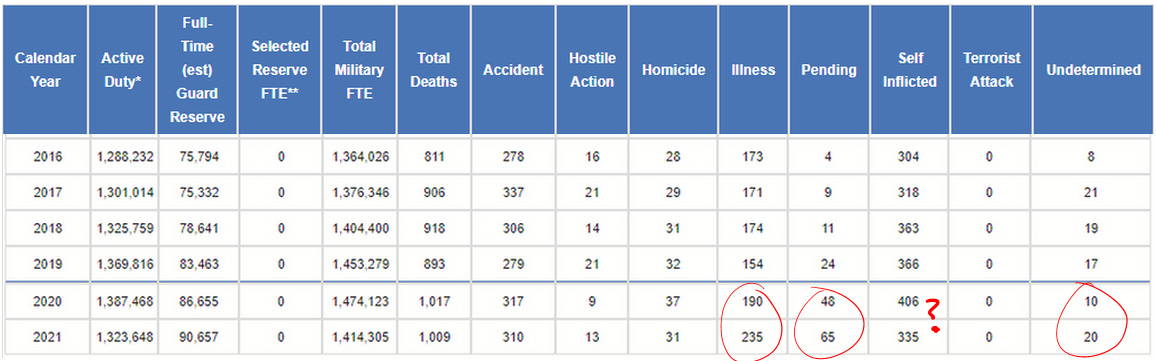
In interviews, I noted that after matching actuarial tables to military age bands, I figured that there would be a bit over 700 non-combat deaths annually in the military. It looks like I was slightly low on account of an elevated number of suicides and accidental deaths, which makes sense given the challenging nature of military service, but otherwise spot on.
Now, let's go category by category through the data that's been released.
Deaths due to illness: These were up 36% in 2021 over the five year average. They were only elevated 10% in 2020. There will be those who make the argument that these jumps are both due to COVID-19, but even if that is true, recall that per case severity of COVID-19 infection skyrocketed along with vaccine administration—both at the outset and also running up to the August vaccination mandates.
Note: This fits with recent research published by Didier Raoult's lab that shows that the vaccinated might present lower viral load and culturability of the virus, but not symptoms or disease severity (Boschi et al, 2021).
Pending causes: It may be that these numbers drop over time, but the 2021 total is substantially elevated relative to prior years. This is consistent with what we know about R-code (R99) mortality data.
Undetermined: It's unclear what the difference is between these and "pending", but these might all be lumped as R-code mortality data, but the "undetermined" may be a more permanent category.
Self-Inflicted (suicides): This one has me scratching my head. The DMED queries show increases in suicide ambulatory and hospitalization reports both in 2021, but a merely small uptick in 2020 in hospitalizations.
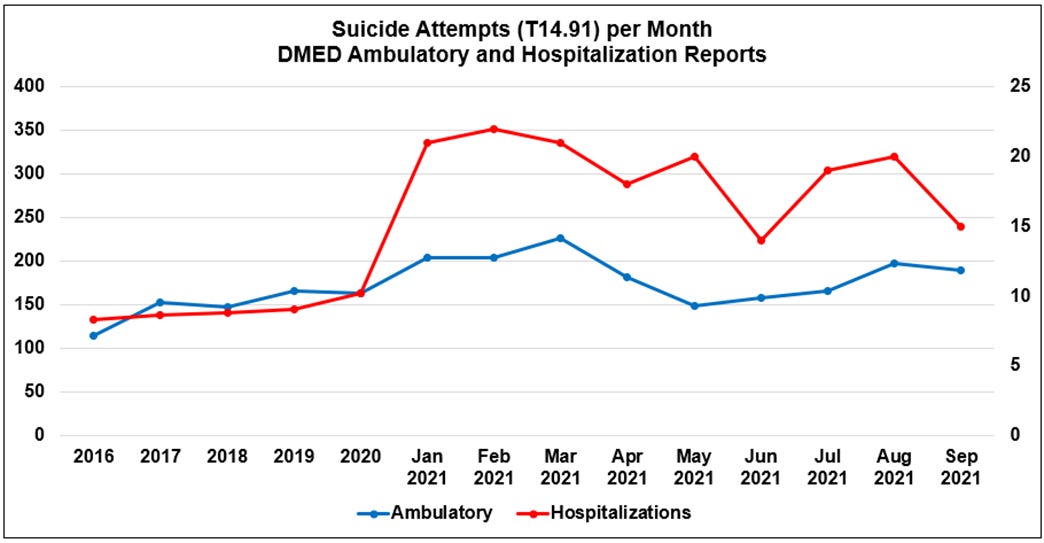
These are not the same as fatalities, sure, but it would shock me if they do not correlate with fatalities. But the just-released military mortality data shows that suicides were at a peak in 2020, but at a lower and moderate level relative to recent years during 2021. However, everything I'm hearing from military personnel and seeing in media reports suggests that suicide became a large problem after the vaccine rollout.
The Ungovernable Armed Forces?
In the meantime, the Chair of the House Intelligence Committee, Adam Schiff, is busy trying to codify into the National Defense Authorization Act (NDAA) a prohibition on the use of information, such as the DMED queries from the four whistleblowers, as "evidence in any trial, hearing, or other proceeding in or before any court, grand jury, department, officer, agency, regulatory body, legislative committee, or other authority of the United States, a State, or a political subdivision thereof."

I'll refer to this as the Military Industrial Complex Achieves Orbit (MICAO) Amendment as it seems to make the U.S. Armed Forces, and those in their sphere, into an ungovernable branch of government—essentially the only branch of government that matters.
This is what an Authoritarian Coup looks like. This is one of those moments when you should call your Rep and say, "No, absolutely not," and maybe add, "Stop 98% of that other crap going on, too."
Surely the MICAO Amendment is unconstitutional. Then again, how long would it take to strike it down once enacted? Part of what we're facing seems to be something like a Distributed Denial of Service (DDOS) attack on representative governance and citizens that would do anything to protect the liberties of citizens. We are being inundated with disturbing, unconstitutional laws and bureaucratic absurdities that are too numerous to fight in any sort of unified way necessary.
It's almost like the [honest portion of] the libertarians were right: Letting government become this large and centralized is a critical failure in losing control of institutions.
Do we have enough representation capable of pushing back against any of this?
On March 7, 2022, Senator Ron Johnson sent a letter to Unissant, the firm contracted for handling the DMED, requesting information related to the glitch. From that letter:
I was disappointed to hear of Unissant’s refusal to provide information informally about its management of DMED. Because of the concerns and unanswered questions relating to the potential increases of medical diagnoses in DMED, as well as the alleged data issues on the system, I hope Unissant will cooperate with this Senate examination and respond to this formal request for information:
Please explain Unissant’s contractual obligations with managing data in DMED. Please provide all contracts with government entities concerning this relationship.
Is Unissant aware of data issues on DMED? If so, what are those issues, when were those issues uncovered, who uncovered those issues, and to what extent did Unissant communicate those issues to DoD?
Please list all other instances where issues were found in DMED (e.g. data corruption).
Please provide all documents and communications between Unissant and DoD referring or relating to DMED from Aug. 1, 2021 to present.
Finally, I request Unissant preserve all records referring, relating, or reported to the Defense Medical Epidemiology Database.[8] Please immediately confirm to my office the completion of the records preservation and provide all other responses by March 21, 2022.
Thank you for your attention to this matter.
While Senator Johnson is doing more than just about anyone in Washington to shine a light on the twisted problems of the pandemic, this is a prime example of why I am frustrated that my findings were not more broadly shared or used as Square One for immediate investigation. Just one or two meetings would have made this letter more effective, and wasted less time, but I was not even made aware that the whistleblowers had shifted lawyers until weeks after this letter was crafted, and my attempts at convening a meeting with seemingly interested parties and Thomas Renz went ignored back in February. The time scale of the Johnson request needed to be rolled back—probably to the start of the entire vaccination program, if not earlier. The May 2021 MSMR was already published by August 1, 2021, and that is where the primary problem lies—not the glitch. By August, the DMED had already been manipulated, and should be viewed as a fake with respect to the 2016-2020 data.
Please Support These Investigations
I've taken a few hundred hours of time to work on this project, and make the information and results free to all viewers. Paid subscriptions are necessary to keep this work going. Please consider subscribing or giving a subscription as a gift. It makes a difference in what we are able to accomplish.
I’m surprised you didn’t get the first call when they stopped publishing this data. They didn’t call me either. Very strange indeed!!
So. I think your observation is another indication we are dealing with an adaptable and not yet beaten adversary. Renz lets the cat out of the bag, then you make the threat very clear, so they fix that vulnerability… We see since omicron the emergency evaporating such that breakthrough data and VAERS reporting is drying up.
Don’t worry, all’s fine. We’ll send you bogus test kits made in the COVID Mother Country so you can quietly keep your breakthrough infection to yourself! We’ll ease things up and let you take your masks off for the summer! The situation is more stable now. We’re going to close up shop on our State covid dashboard, and stop doing all this terribly manpower intensive data reporting… Sure you’ll understand… (but emergency apparently not dwindling to the point of not subjecting kids to the jabs and not preserving neverending EUA’s).
Freedom of data availability is what has allowed voices like yours, Dr Rose, Joel Smalley… bring forth solid data backed objections to the first rounds of mandates. Now maybe they’re licking their wounds and patching holes in the walls they didn’t think to close in that first try?
Been looking at the evaporating VAERS data lately and not cynical at all 😉