


Defining Away Vaccine Safety Signals 5: The DMED "Glitch" Revealed?
The Vaccine Wars Part XXVI

"It is the common peoples' duty to police the police." -Steven Magee
Friday, March 11, attorney Thomas Renz was back in court. He presented the first piece of my DMED analysis. Today he posted a press release that includes my affidavit suggesting the high likelihood that the DMED data was doctored by somebody at the DoD.
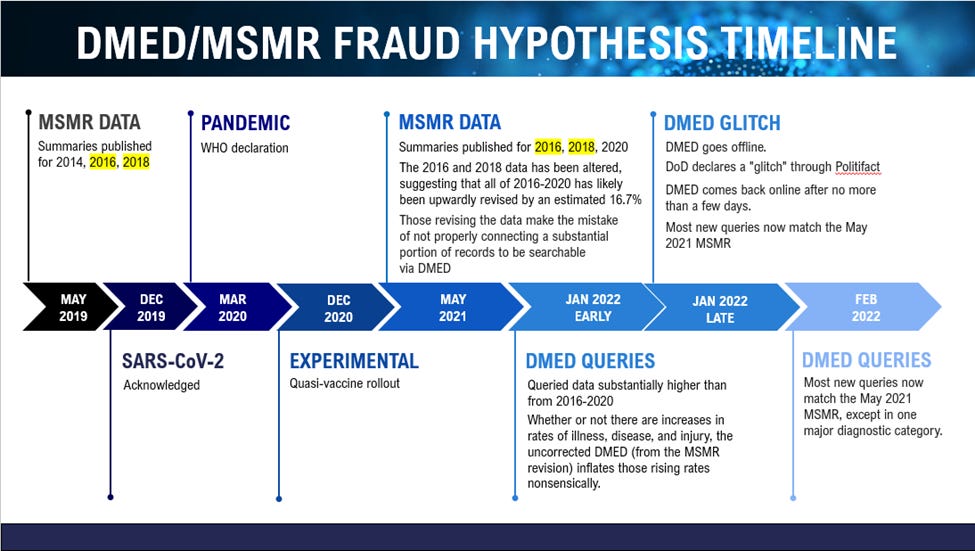
Recall where we were with this story a month ago:

Since then, I have devoted several weeks combing through data from the Defense Medical Surveillance System (DMSS) via the Defense Medical Epidemiology Database (DMED) and other sources. Understand that these numbers will change in a final report, but that's not because the whistleblowers did anything wrong, or because there are no signals of harm from the experimental quasi-vaccines. There are plenty of clear signals. And what I suspect took place with regards to the data looks far uglier for the Department of Defense (DoD), or at least those responsible for the medical data.
This is going to take some time, and multiple articles, but I will do my best to explain it all. Understand also that I'm holding back a lot for now. It is unfortunately necessary to see how the DoD responds before showing our full hand.
Pharmacovigilance Connections
Before we move forward, I want to lay out a little context for readers wanting to understand the Big Picture of vaccine safety (pharmacovigilance) signal monitoring and analysis. According to the CDC, the Department of Defense (DoD) is one of the several sources of information used to assess vaccine safety. While not specified in the slide taken from this February 2022 report, this certainly means the DMSS and DMED.
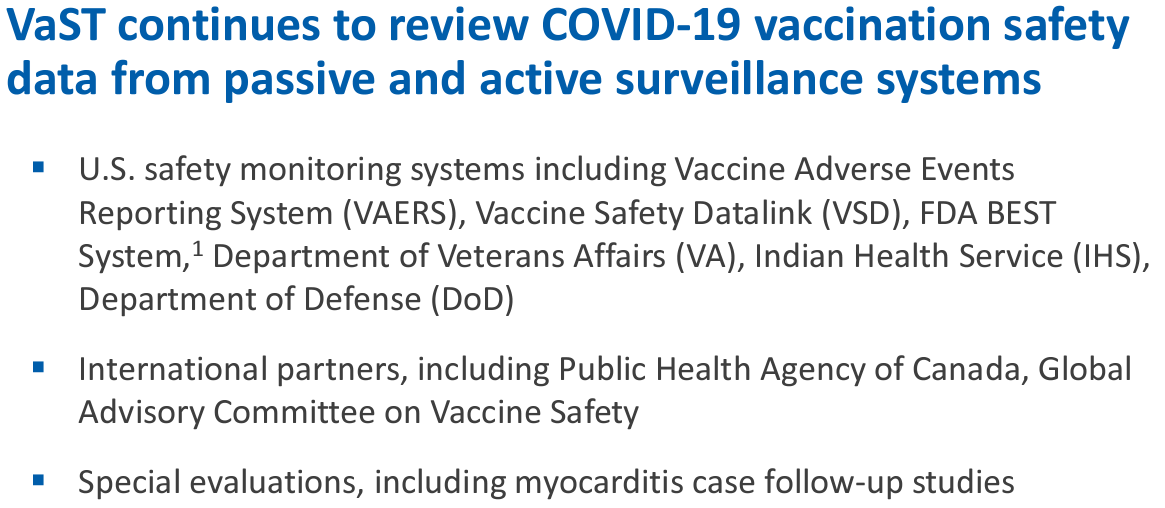
In short, this means that the CDC has an active data relationship with those running the DMSS and DMED, for the purpose of passive monitoring. Note that "passive monitoring" does not preclude active communication and planning.
Was There a "Glitch" in the Database?
You might as well ask Bill Clinton what the definition of "is" is. Certainly the numbers in DMED underwent a massive "update" in late January, and these updates dramatically raised the quantities and rates of illness in query outputs across the board both by medical category and also by years 2016-2020. This data revision was almost uniform in nature, like a factor of around 3.3 was applied almost uniformly to every one of thousands of possible outputs during that five year span. If there was a glitch, it was the kind of glitch that doesn't play favorites, which narrows significantly the potential nature of the glitch.
Most glitches do play favorites, but let's not dwell on that for the moment.
In order to better understand the data, my team located published summaries of historical data to compare the new (post-glitch) numbers with. The Medical Surveillance Monthly Reports (MSMR) are publicly available at Health.mil.
https://health.mil/Military-Health-Topics/Combat-Support/Armed-Forces-Health-Surveillance-Division/Reports-and-Publications/~/link.aspx?_id=534E26BD8E5D4ECC8CAA8ABA47679691&_z=z

The monthly reports cover a variety of health-related topics using data from DMSS/DMED, and perhaps other sources. Every May, the MSMR includes three annual summaries of both ambulatory and hospitalization data for three prior years staggered with a year in between. For instance, the May 2021 MSMR included summary data for the years 2020, 2018, and 2016.
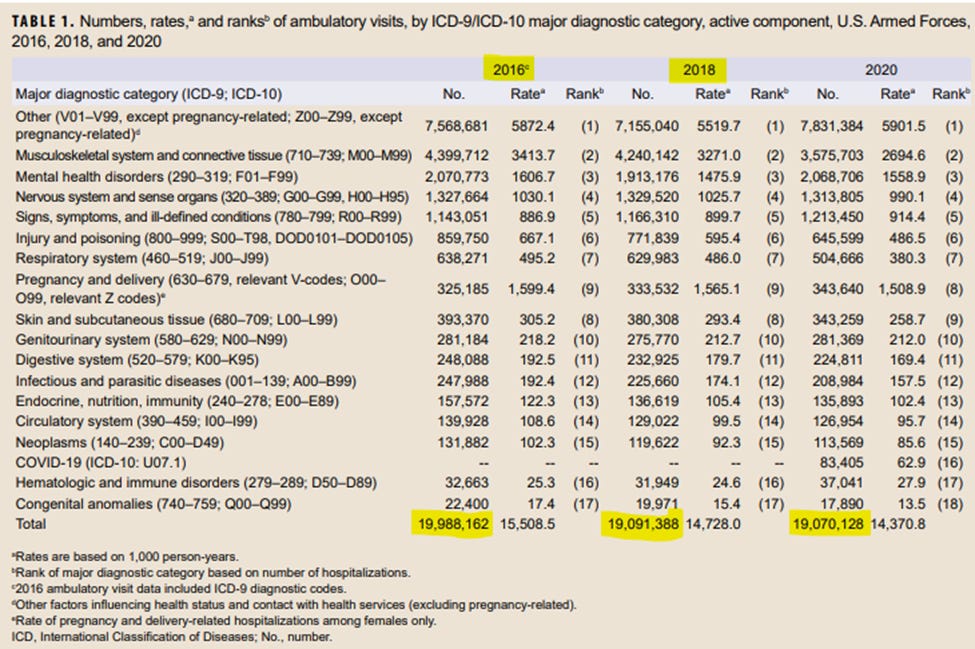
Source: May 2021 MSMR, Vol. 28 (No. 5), p. 18
Readers interested in learning more about the old ICD-9 codes and the newer ICD-10 codes used in medical reporting can start here.
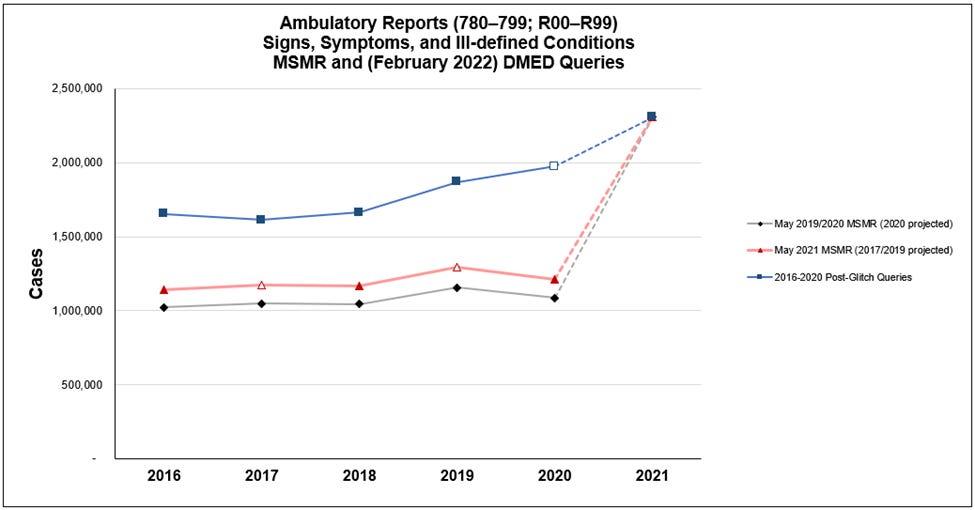
We took all of the past decade's worth of ambulatory and hospitalization data for each broad medical diagnostic category and organized it into spreadsheets. Something stuck out in the ambulatory data in particular—large revisions in the ambulatory data between May 2019 and May 2021 MSMR editions.
My first thoughts and questions were
Nobody revises a database (particularly one this important) without clear documentation for users of that database. The very idea is preposterous. Rates of illness and disease just changed. Didn't somebody think that doctors and researchers who use DMED ought to know about that? Video game makers do a better job of communicating database updates.
Do we ever see such changes between any other May MSMR annual summary reports? Is this revision historically unique?
Why don't we see associated revisions in the hospitalization data?
With respect to Q3, I suspect that,
Hospitalization data is harder to fake due to standardization and formalities of record systems.
Many elevated illnesses observed in 2021 may not (yet) require hospitalization.
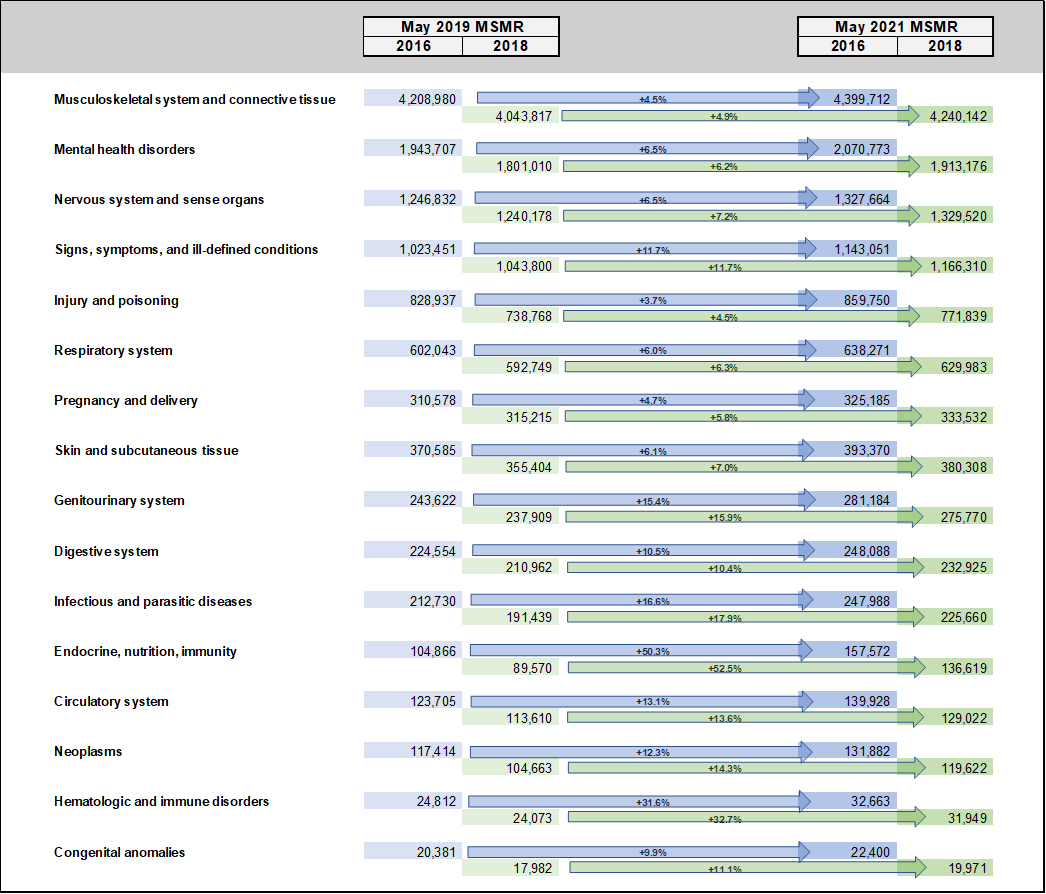
With respect to Q2, the answer is, "No, not ever." The average change within one of the summary diagnostic categories turns out to be 0.1% (likely mild record updating), but the average across the 16 most common diagnostic categories (defined by ICD-10 codes) was 13.5%.
You can check the 2016 and 2018 numbers from the May 2019 MSMR yourself to follow the revision.
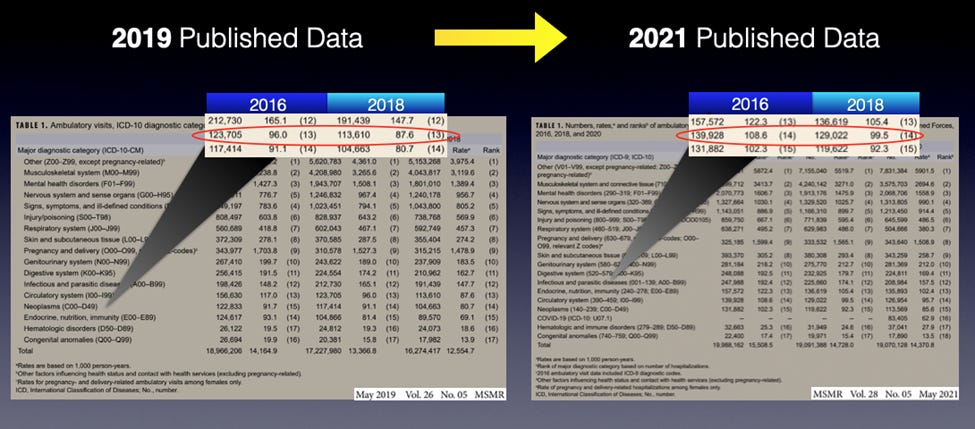
Here is a visualization of the scale of the summary revisions.
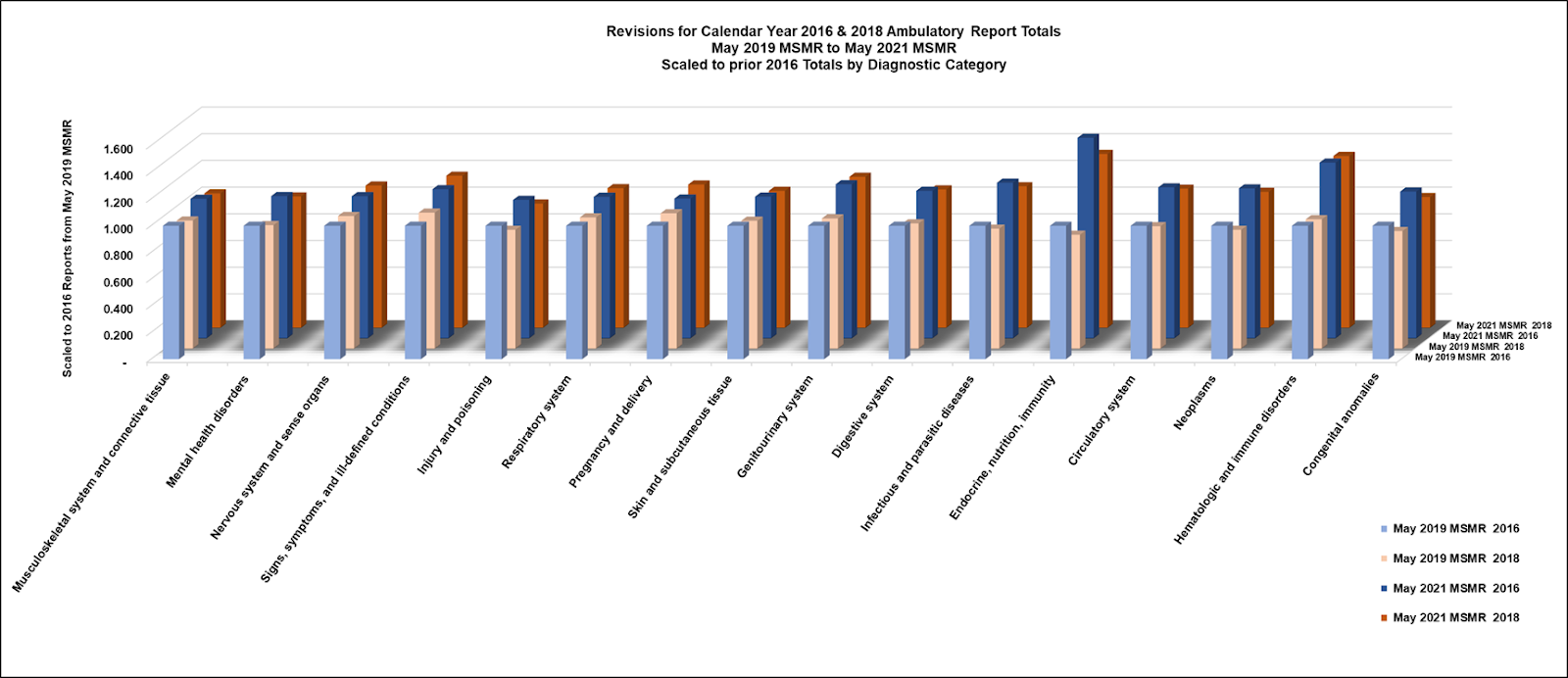
While the May 2021 MSMR appears to list additional ICD codes, these are previous versions (ICD-9) of the same codes (ICD-10), so that does not explain the elevation of disease and injury rates between the publications. All but two of the diagnostic categories remained consistent in ICD-10 coding. The largest category “Other” added V-codes which includes pedestrian and traffic accidents, so we ignore this category in our first order inspection and analysis.
Given the observation of the large revisions, it is not simply unprecedented, but shocking to see neither asterisk(*) nor explanation in the MSMR for such large changes. Given the importance of the data, anyone interested in the data would certainly want to understand the nature of the changes. It is not simply implausible, but defies belief that such a shift in publication would take place in a casual and disinterested manner.
The nature of these changes needs to be understood, but it is incumbent upon anyone concerned with the health of the U.S. military (and to every American) to ask whether these revisions represent fraudulent data engineering.
On May 25, 2021, Acting Assistant Secretary of Defense (Health Affairs) Dr. Terry Adirim and Defense Health Agency Director, Lieutenant General (Dr.) Ronald Place addressed the House Appropriations Defense Subcommittee. In their discussions of the Military Health System (MHS), including specifics related to the COVID-19 pandemic and experimental quasi-vaccines. They did not mention or explain anything like a massive update of the data in the DMSS or DMED, though the opportunity would have been important and timely.
Hypothesis: The "Glitch" Was an Artifact of Data Fraud
The May 2021 MSMR was published with summary data for years 2020, 2018, and 2016 at a time when some data for the year 2021 was already known. I think that somebody saw signals of damage by the experimental COVID-19 quasi-vaccines and panicked. It is likely that data for all years 2016-2020 was then upwardly revised to look more inline with expectations for 2021, though changes in 2017 and 2019 will not be apparent until the May 2022 MSMR is published (we get to see in a few weeks). Since 2020 data was published for the first time in the May 2021 MSMR, there is no reference to check, but it stands to reason that changes were applied in a relatively uniform manner across these years, which represent all years since the changeover from ICD-9 to ICD-10 medical codes as used in the DMSS and DMED.
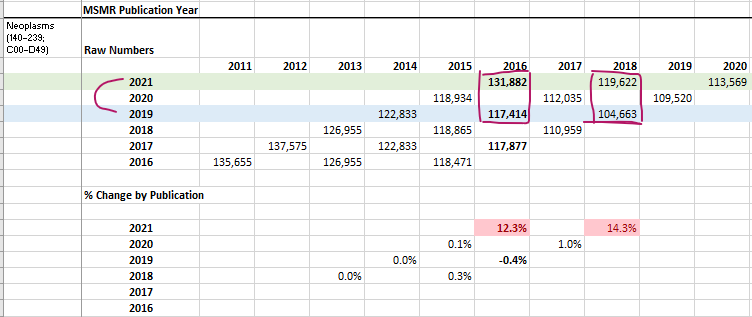
We did check to be sure that the MSMR data should pass through faithfully to DMED. We compared the 2021 MSMR (red) totals by diagnostic category to queries from DMED run January 31, 2022 or later, and found close matches for all but one major diagnostic category, which is "Signs, Symptoms, and Ill-Defined Conditions (R00-R99)", which seem to have been revised upwardly again since the May 2021 MSMR. Here is the comparison for Neoplasms (cancer):
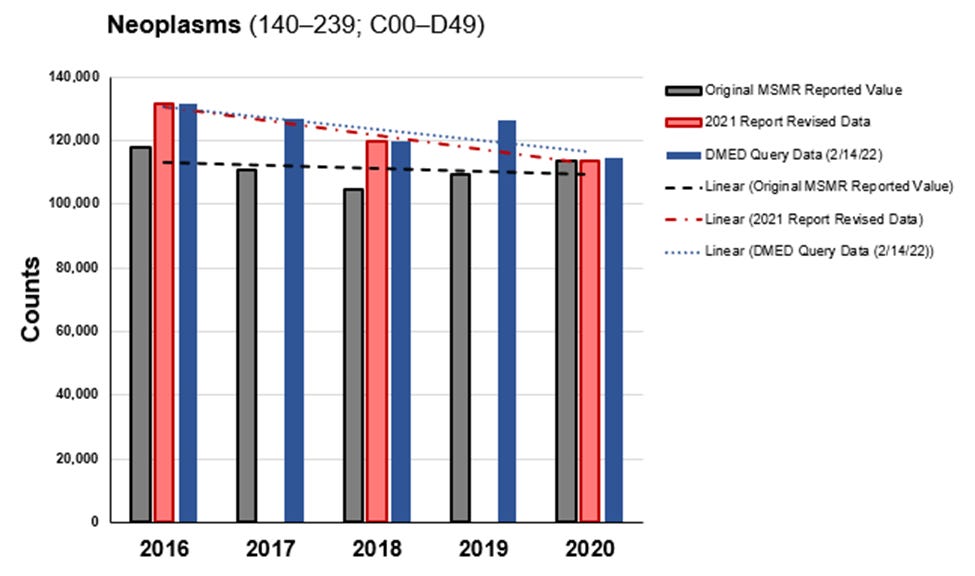
I plan to publish these graphs for all major diagnostic categories in the future, but suffice it to say that the most recently published MSMR reports are almost identical to recent DMED queries in all categories except for one. I'll get to that…
Signs Consistent with the Data Fraud Hypothesis
In many cases, illnesses understood to be associated with the experimental COVID-19 quasi-vaccines were upwardly revised at much greater rates than for the broader diagnostic categories. For instance, ambulatory reports for 2016 and 2018 were upwardly revised 21.2% for all illnesses associated with the Circulatory system (ICD-10 I00-I99). However, total ambulatory reports for myocarditis, pericarditis, and hypertensive disease were upwardly revised by larger amounts for those same years:
(I40) Acute Myocarditis: Revised upward 48.3% (2016-2020)
(I30) Acute Pericarditis: Revised upward 99.5% (2016-2020)
(I10-I15) Hypertensive Disease: Revised upward 2381.3% (2016-2020)
There are numerous other examples that will not fit in one substack post.
As I alluded to before, the one major diagnostic category that appears to have been revised a second time (and dramatically) is "Signs, Symptoms, and Ill-Defined Conditions (R00-R99)", which is a category that includes conditions with unknown etiology. Many physicians likely toss vaccine adverse events and injuries that they do not yet understand into this category.

Not only were the R-codes upwardly revised substantially between May 1, 2021 and Jan 31, 2022, but the totals now look like a trend where the higher totals in 2020 and 2021 could be plausibly blamed on COVID-19.
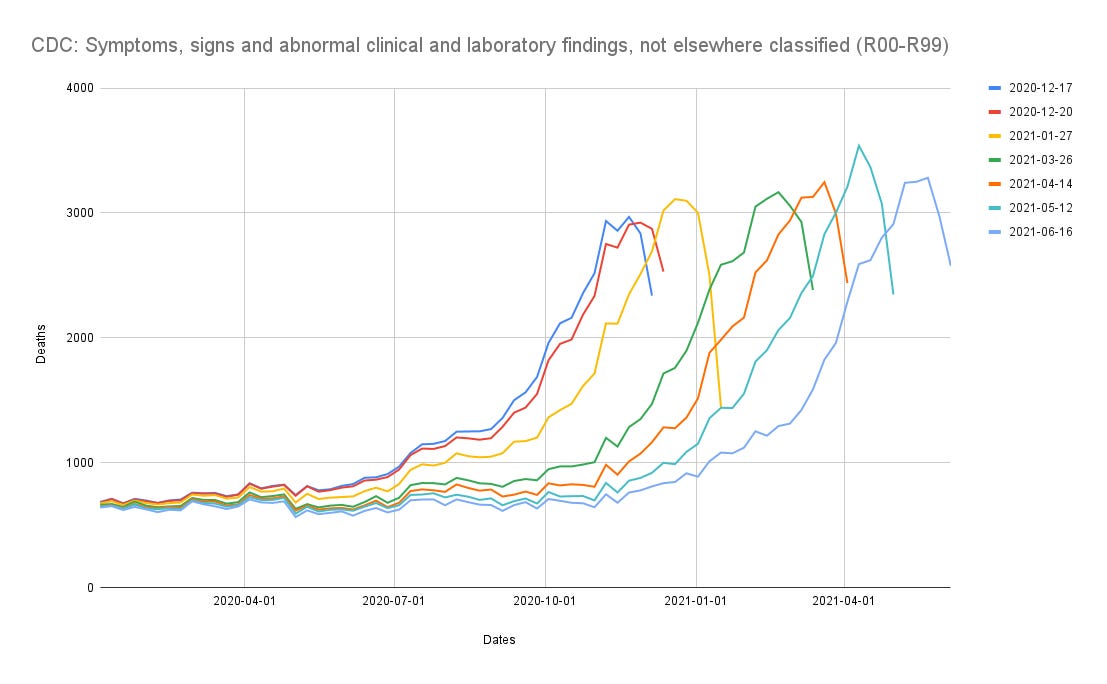
We will talk much more about the R-codes in future articles. But I wanted to point back to both Joel Smalley's Massachusetts analysis, here:

The R-codes in Mass. are stuffed full of (all cause mortality) R-codes, and this blog post by Austin G. Walters shows rising mortality totals among the R-codes:
While I wanted to run a more continuous analysis on rates of illness further back in the past, understand that such a project would be very time consuming, and my team is currently too small to study all avenues. The changeover from ICD-9 to ICD-10 codes adds a hurdle to that process. The more standardized is the data, the easier and clearer is the analysis. Take that as an understatement.
Ruling Out Other Hypotheses
The idea that dramatic changes in medical reporting data would go unexplained already pushes all limits of credibility. But let us also give consideration to other explanations for the large scale changes that we see in the data.
Other hypotheses that we might entertain with respect to the supposed glitch include the addition of “lost-and-found” hospital data, but the revisions to the hospitalization data between the same 2019 and 2021 MSMR were only revised around 0.5% (none at all were large), which is lower than average 1.2% upward revisions observed in publications back through the May 2016 MSMR, even spanning a challenging adjustment from the use of ICD-9 to ICD-10 coding.
One way or another, we'll have to see what the DoD claims about the dramatic and unexplained revisions in DMSS/DMED via the MSMRs. Perhaps there is an explanation that I haven't considered? Why then was it not offered in May 2021, or in January of this year?
Current Mood: Hulk Smash Data Fraud

Understand that there is so much data to present that this first examination is held brief. We have hundreds of charts showing safety signals that should have been incredibly hard to ignore for anyone who cared to look at the data.
I'd like to thank all the many Rounding the Earth subscribers for the community, financial support, and for tolerating my absence while working on this project. We are all in this together, sharing our frustrations. But at least we're together.
Addendum: Click here for the next article in this series.
I feel an enormous amount of disappointment when I allow myself to ponder how I completely distrust every institution now. I just can’t believe the fraud is that widespread. My Dad went to the Hospital for “Covid” pneumonia (mid 70’s), he refused Remdesivir and asked to only be treated for Pneumonia, he was out in a day. The doctor was so irritated they slapped a DNR bracelet on him (he had no idea what that meant). It just saddens me how malicious people have become. Every institution in our world has proven themselves not worthy of any trust at all.
Amazing dedication and analysis. So glad you’re working for the legal team. Stay safe!