


Bangladesh's Tale of COVID-19, Medicine, and Vaccination
Pandemic National Case Studies

“Half-truth is more dangerous than falsehood.” -Bangladeshi proverb
Other Pandemic National Case Studies can be found here.
The almost uniformly Bengali and Muslim nation of Bangladesh celebrated its fiftieth anniversary last year, the result of a culture-driven governance split, and eight months of military clashes with also-Muslim Pakistan. Pakistan itself had split with largely Hindu India in 1947 when Great Britain still had a hand in drawing the boundaries of Asia.

Supporting a population of 170 million, Bangladesh is the eighth largest nation in the world by population with an economy that has doubled roughly every decade since 1960. However, while the Bangladeshi domestic economy is growing, including its education and technology sectors, all that depends on a massive and energy-starved clothing production sector that provides most of the nation’s income from exports to the U.S., Europe, and select nations in Asia. Since Bangladesh now imports a bit more than the sum of its exports and foreign remittance earnings, Bangladesh, a nation which has brought tens of millions of its citizens out of poverty in recent decades, stands at a crossroads.
During the pandemic, less data has emerged from Bangladesh in a timely manner than from many other nations, but we will work with what we have to go on.
Bangladesh’s Experience With Early Treatment Medicine During the Pandemic
When COVID-19 hit Bangladesh, physicians there immediately turned to hydroxychloroquine (HCQ), the two largest producers of which are neighboring India and Pakistan. Shortly thereafter, Bangladesh added ivermectin (IVM) to its treatment choices after an in vitro study out of Australia (Caly et al, 2020) showed that IVM stops SARS-CoV-2 viral replication.
A case series of 100 COVID-19 patients put on HCQ published out of Bangladesh (Tarek Alam et al, 2020) showed no hospitalizations or deaths, and a controlled trial showed patients receiving IVM achieving far faster viral clearance and reduction in hospitalization length of stay (Khan et al, 2020). Another smaller randomized controlled trial found that patients using IVM achieved faster viral clearance (Ahmed et al, 2020) than those who did not receive the drug. Bangladeshi researchers sought to test the drugs against one another. Unfortunately, the study included a mostly young population (low risk means low powering of such a trial) and the results did not show a significant difference in time to recovery between the two groups (Chowdury et al, 2021).


Though Bangladeshi physicians and medical scientists published numerous papers on the effects of HCQ and IVM, there is poor aggregate data on the use of the medicines. But we know that both drugs were used to some degree to treat patients throughout the early months of the pandemic. And Google search results confirm that.


YouTube seems not to have fully censored this story.
During that time, Bangladesh suffered fewer COVID-19 cases and fewer deaths (both per million population) than most of Asia and the rest of the world.
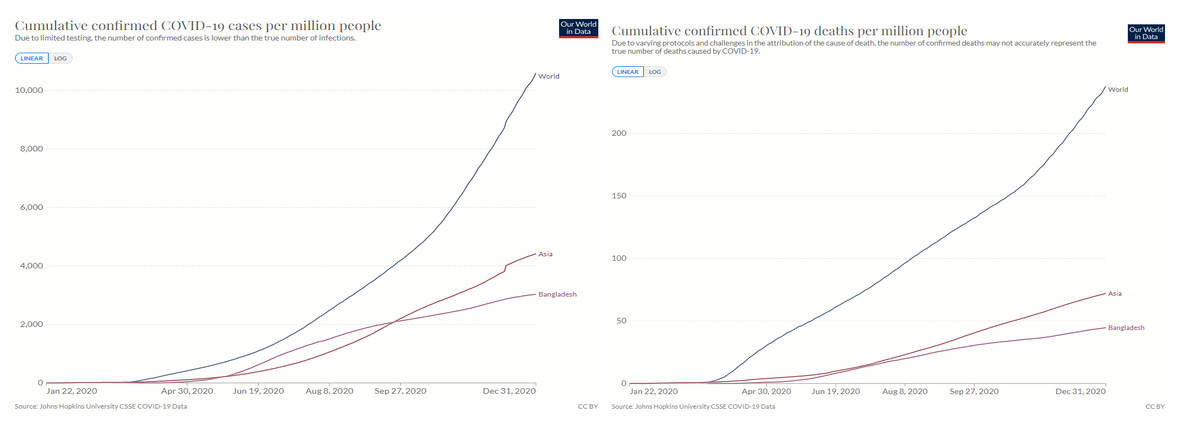
Not bad for the single most densely populated nation in the world with a population over 8 million!
Bangladesh’s Experimental Mass Vaccination/Transfection Program
Despite suffering among the lighter epidemics in 2020, Bangladesh chose to start vaccinating its population in 2021. While the vaccination program began on January 27, 2021, it wasn’t until July that the program ramped up, perhaps due to the global availability of vaccines.
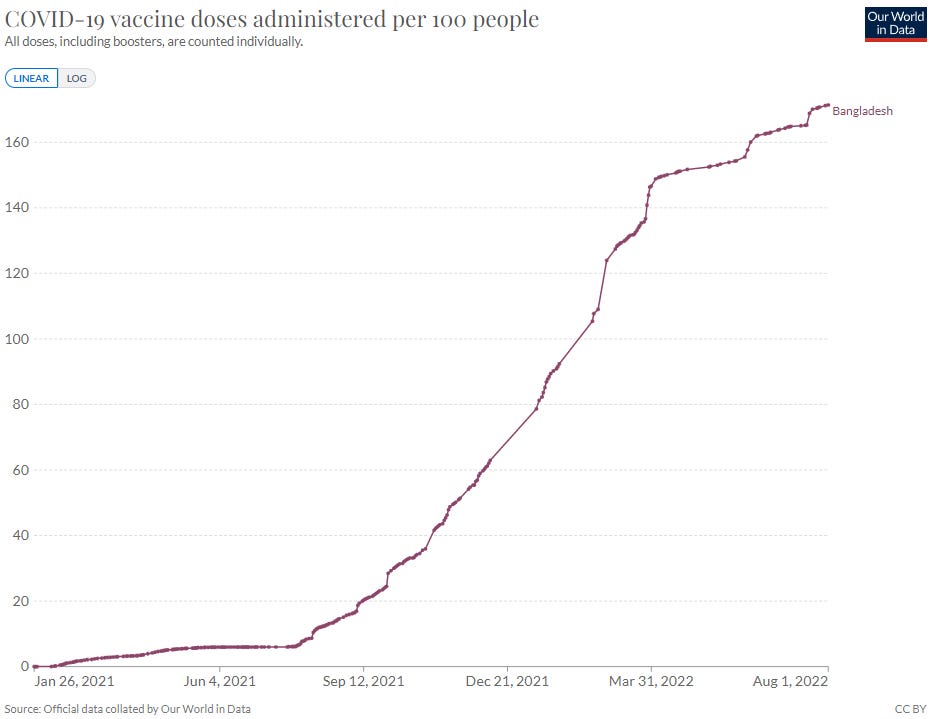
The vaccination surge came when the U.S. gave over 73 million doses of Pfizer, Moderna, and Johnson & Johnson vaccine doses to Bangladesh, free of charge.
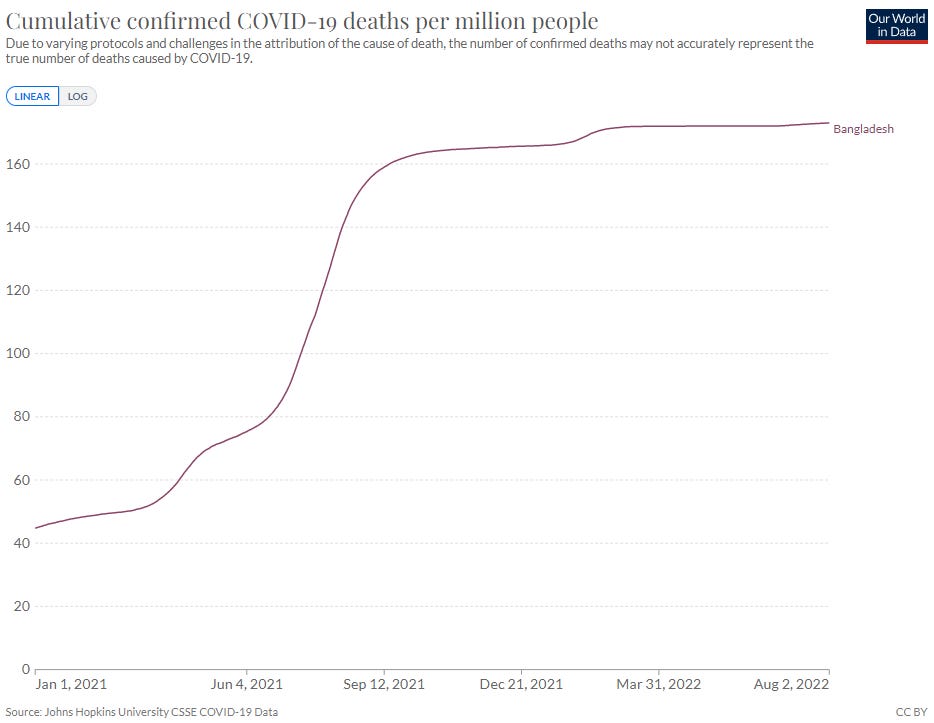
Almost three-quarters of Bangladesh’s COVID-19 deaths have occured since the outset of the vaccination program. But since the large-scale vaccine delivery program began after COVID mortality began to soar during the Summer of 2021, it is hard to see any association at all, positive or negative, between the vaccines and the overall disease impact.
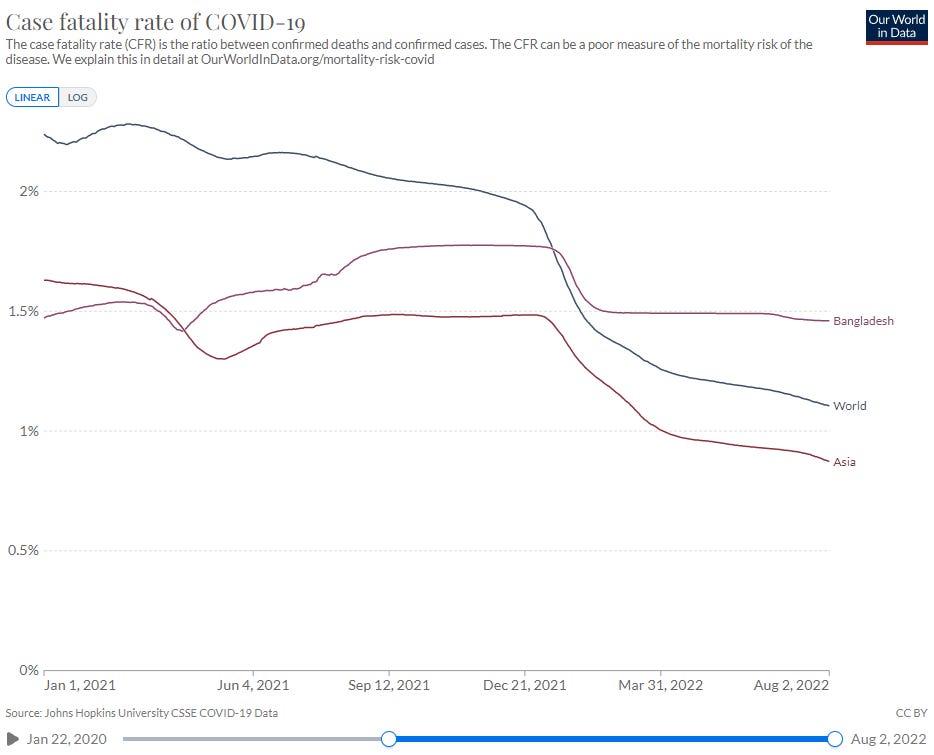
If we focus on Bangladesh’s case fatality rate (CFR), which is the ratio of deaths to cases, we note that Bangladesh’s CFR is unchanged since the end of 2020, whereas CFRs elsewhere in the world largely fell, and Bangladesh’s rose a bit during the heavier portion of the mass quasi-vaccination experiment.
Fortunately for Bangladesh, the mortality impact of COVID-19 is remains less than a quarter of that of the world average. While it might be illuminating to observe Bangladesh’s excess mortality data, I was unable to locate it online. If a reader knows where to find it, I will update this article.
It is noteworthy that Bangladesh joined the chorus of criticism and pushback against the World Health Organization’s push to assume sovereignty over nations in the event of health emergencies (which may be politically defined).
Like many nations, Bangladesh is currently in the midst of an energy crisis. Parts of Dhaka are seeing multi-hour blackouts to shed load on the immense city’s power infrastructure, which in turn affects the textile industry. Students are protesting the cost of fuel, but who can fix the supply chain for them? Competition for gas with Europe has led to a steep decline in foreign reserves, putting stress on the nation’s banking network. Now they reach out to the IMF, World Bank, and the Asian Development Bank.
Will one nation after another go into deep debt to the world’s largest banks?
Also causing trouble is one man’s insistence on singing. Singing poorly, but freely. Enjoy your moment of zen.
The Dr. Been video is interesting. I was not aware of Dr. Been until 2021, when he appeared to be fully on board with the vaccination program. He was resistant to the biodistribution of the vaccines outside the deltoid muscle and lymph nodes, and was very reluctant to question the "safety and efficacy" of the vaccine. I was not happy with that and stopped watching his videos.
In the linked video, he speaks favorably of not just Ivermectin, but of early treatment in general, particularly of hydroxychloroquine and of mixing doxycycline with the Ivermectin treatment. In the absence of a drug or "vaccine" approved by the FDA for treatment of Covid-19, Dr. Been spoke in favor of doctors using their skills. However, as EUAs became available for the "vaccines" and Remdesevir, he seems to have stopped pushing early treatment. This is why YouTube tolerates him. Whether someone "got to" him or he was always going to endorse the official narrative, I don't know. But early on, he was for early treatment and saving as many lives as possible given the tools doctors had at the time. He built a loyal following and many continue to see him as a truth teller, quite useful for the official narrative.
I don't judge Dr. Been, but at this point I pay him little mind.
Interesting you should mention Pakistan as being a major producer of HCQ, because both Pakistan and Bangladesh have extremely low Covid deaths per million compared to European countries, Israel and the US. I'm talking 10 to 20 times lower rates.
Also, CFR is a very poor metric. It ignores the fact that unvaccinated people are less likely to test and report. I ran a survey here in New Zealand and 90% of the unvaccinated i polled did not report their Covid status to the Ministry of Healths data tracking system.