
Understanding Batch Lot Toxicity
The Vaccine Wars Part XVI

"Research is something that everyone can do, and everyone ought to do. It is simply collecting information and thinking systematically about it." -Raewyn Connell

I have largely stayed out of the bad batches/hot lots debate. But an article that a friend found caused me to revisit the topic, and I'll share my thoughts now.
Forgive me, but because the difference between a batch and a lot is irrelevant to the points I make in this article, I'm going to pick one term (casually), form an acronym, and run with it. When that discussion first began, I was skeptical of the hot lots hypothesis (HLH). I will discuss why that is the case, but also the importance of investigating the hypothesis as well as a very real set of vaccine risks that we should always keep an eye on.
I will borrow a graph from my friend Jessica as a numerical reference for some discussion.
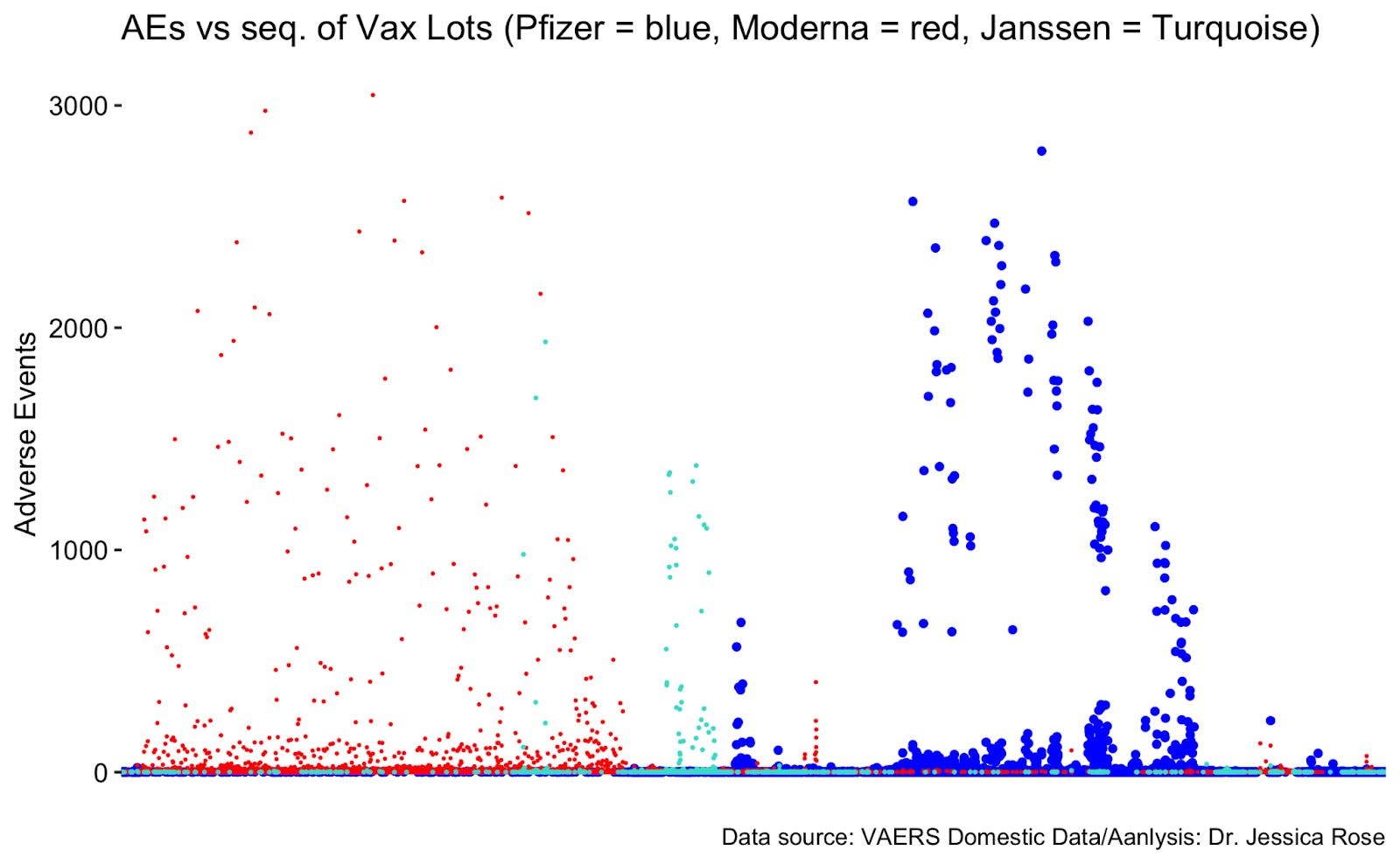
What we see is that some vaccine lots seem to have as much as three orders of magnitude of reported adverse events (AEs) above the safer lots. This brings me to my first point:
Differentials in reported AEs do not necessarily imply differentials in AE risk.
Is it possible that some lots are given at locations where AEs will be more likely to be reported?
Of course! There is far more monitoring of dose recipients in long term care, for instance. There are also political and geographical biases that could (and likely do) play a role in whether a particular AE gets reported to VAERS. When I think honestly about those biases, I could easily imagine those stacking to a range of something like 0 to 2 (think like a confidence interval) orders of magnitude. While I doubt there are many situations where reporting bias results in 100 times as many AE reports, we see in the plots above that the "hot lots" are rare.
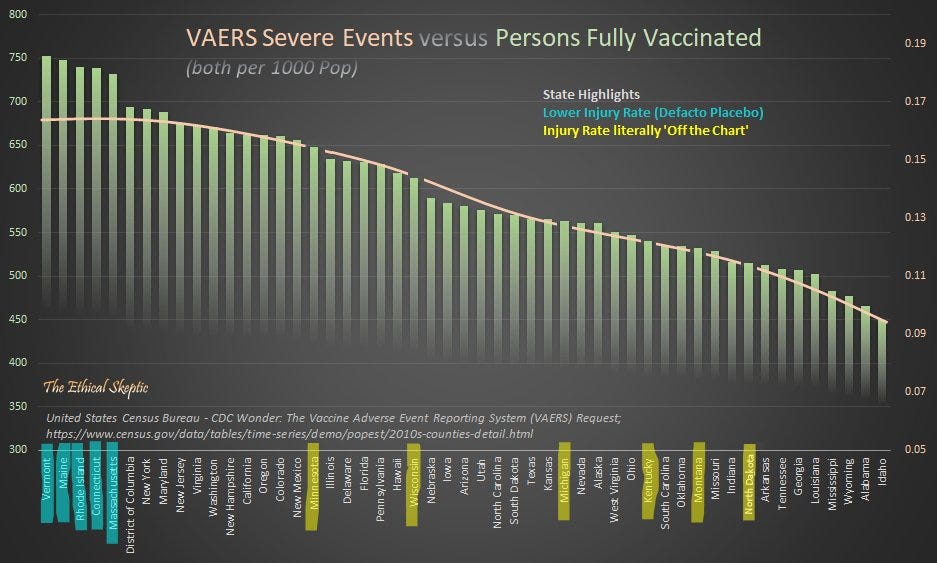
The Ethical Skeptic graphed state AE data, and when I look at this graph, I think, "This fits my guess that medical staff would feel more comfortable reporting AEs in red states and less comfortable reporting AEs in blue states." The states at the tails are mostly smaller states where we would expect higher variance, and zooming in more locally we might expect further ratio extremes.
Next,
Lots may simply be associated (correlated) with AE risk (age in particular).
I suspect that it is often the case that most everyone vaccinated at a nursing home or hospital gets vaccinated by one or a small number of lots. Again, I can easily imagine 0 to 2 orders of magnitude difference between the kinds of AEs that would more often get reported (more serious or irritating AEs likely have a higher reporting rate than mild bruising or itchiness around the injection site).
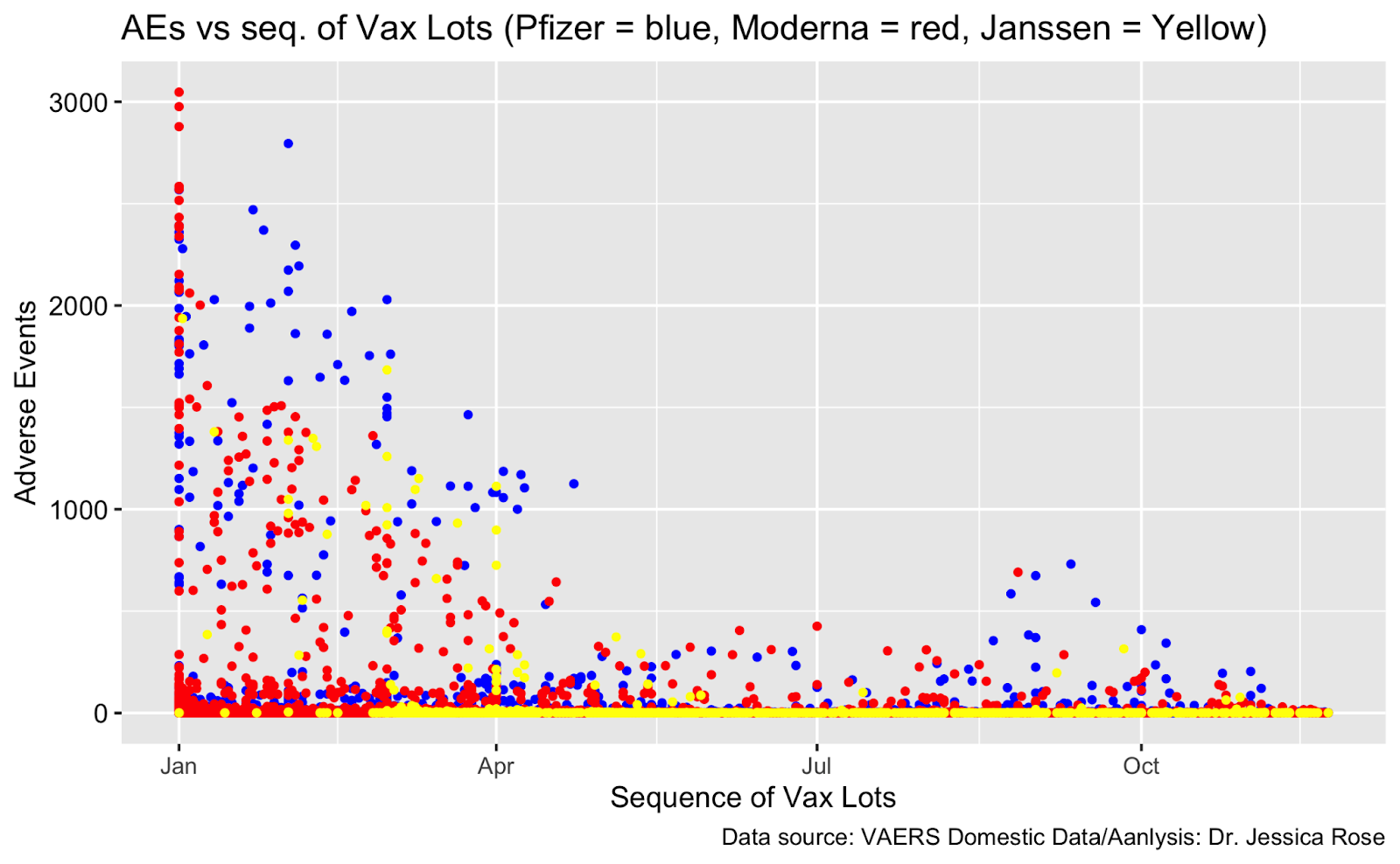
Jessica produced a nice plot showing that the potentially hot lots usually happened earlier in the vaccination campaign where we would assume there is high correlation with age of the dose recipient.
Other Potential Correlates.
I personally suspect that aspiration does correlate with vaccine AEs, and the training of vaccine delivery is likely clustered so that some lots are delivered by only or nearly only individuals who aspirate while others are delivered by only or nearly only individuals who do not aspirate during the injection procedure.
Taking just these considerations (and perhaps those I haven't thought of) into account, I can easily imagine data that appears to suggest "hot lots", but ultimately represents other issues of varying concern. While this certainly does not fully dismiss the HLH, our simplest and primary reasons to be skeptical of the HLH could potentially explain all of the observed effects. However, we should thank all of the investigators looking into this problem, both because the HLH may yet turn out to be true, but perhaps more importantly because that investigation may help shed light on other serious issues.
Not all batch and lot sizes are the same.
It is tempting to presume standardization of such metrics. However, that just isn’t the case, and we need to keep that in mind and account for it in any model before declaring a quantitative result.
Zooming in on Toxic Batches
Of course, we never have to make up our minds fully about a hypothesis where the evidence seems debatable by reasonable minds (mine is not particularly close to being fully made on batch toxicity most generally). To the extent that a potential problem is important, we can continue to study it actively. That's what Craig Paardakooper is doing at howbadismybatch.com. Perhaps some of you can help out with that research.
Poking through his notes, I see that Moderna batches 20A and 21A resulted in the greatest number of AEs, with the 26 batches with the greatest number of AEs all coming from 20A. If these batches were delivered early during the pandemic, and given Jessica's temporal plot, that would have to be the case, then that's nothing new. In fact, it seems to be the case that even within these batches, those delivered earliest resulted in more AEs in a way that is well-ordered:
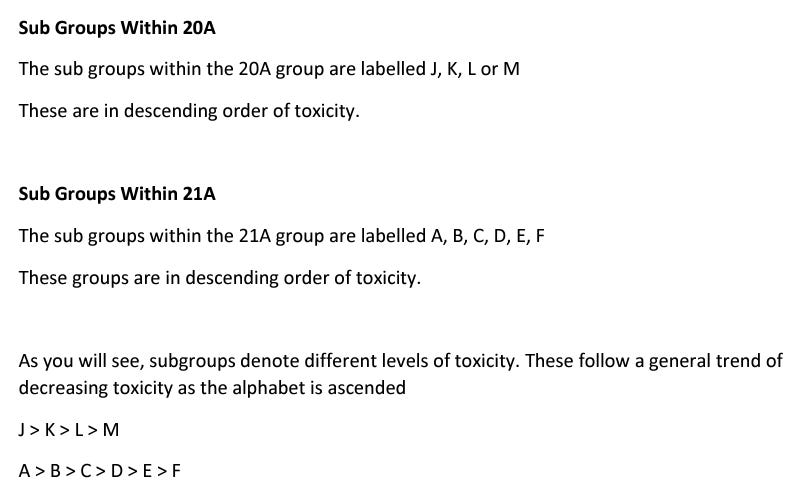
This simplest interpretation still seems to me to be the temporal relationship and its correlation with age of injection recipient.
A History of Toxic Batches
In order to understand the potential for catastrophic vaccine batch defects, let us look back at the so-called "Cutter incident" from early polio vaccine rollouts. In all, 40,000 children were stricken with polio, 200 paralyzed, and at least 10 died due to some mistake(s) in the creation of those particular vaccines.
A few hours ago, a friend of mine posted this blog post by Jon Rappaport from March 13, 2019 into a discussion group. The post covers the interview of a supposed pseudonymous retired vaccine researcher at the NIH. Ultimately, I cannot vouch for the existence of the interviewee, so I am curious if any RTE reader can detect information in the specifics of the conversation that substantiate the story. However, I lean toward thinking this is a real conversation at least partially due to the specific and consistent discussion of bias and misdirection that we've witnessed during the mass vaccination campaign.
A: You are dealing with the basic faulty premise about vaccines. That they intricately stimulate the immune system to create the conditions for immunity from disease. That is the bad premise. It doesn’t work that way. A vaccine is supposed to “create” antibodies which, indirectly, offer protection against disease. However, the immune system is much larger and more involved than antibodies and their related “killer cells.”
Q: The immune system is?
A: The entire body, really. Plus the mind. It’s all immune system, you might say. That is why you can have, in the middle of an epidemic, those individuals who remain healthy.
Q: So the level of general health is important.
A: More than important. Vital.
During the pandemic, I have learned more biology than I'd learned in the entirety of my prior life, but I still feel like I'm climbing the hill in learning about the human immune system—much like a first year graduate student. But one thing that stands out in my conversation with biologists and those who do have a high relative level of expertise is that the human immune system is so vast and complex that no one human being is an expert in all of it. My wife, for instance, does some work in the area of jumping genes in which there are few experts. Few people even know that there is an immune system associated with jumping genes, and even fewer know much about it. So many of the branches of even human biology are still nascent sciences. File that observation away when you listen to the overconfidence in the voices of The Experts of The Science.
But here we get closer to home (for this article):
A: The decline of disease is due to improved living conditions.
Q: What conditions?
A: Cleaner water. Advanced sewage systems. Nutrition. Fresher food. A decrease in poverty. Germs may be everywhere, but when you are healthy, you don’t contract the diseases as easily.
Q: What did you feel when you completed your own investigation?
A: Despair. I realized I was working a sector based on a collection of lies.
Q: Are some vaccines more dangerous than others?
A: Yes. The DPT shot, for example. The MMR. But some lots of a vaccine are more dangerous than other lots of the same vaccine. As far as I’m concerned, all vaccines are dangerous.
Q: Why?
A: Several reasons. They involve the human immune system in a process that tends to compromise immunity. They can actually cause the disease they are supposed to prevent. They can cause other diseases than the ones they are supposed to prevent.
Emphasis mine. Is there evidence to back up this claim aside from just the Cutter incident?
This study published in 2017 found all manner of toxic debris in vaccines.
A few months ago, Japan rejected 1.6 million doses of Moderna's experimental quasi-vaccine amid reports of particulate matter in the vials.
The ministry said later in the day that the substance that had been mixed in may have been metal. "It's a substance that reacts to magnets," a ministry official said. "It could be metal."
In a recent video, former Pfizer Chief Scientist Mike Yeadon provides some. This screen grab of one of his slides shows a couple of influenza vaccine outlier batches.
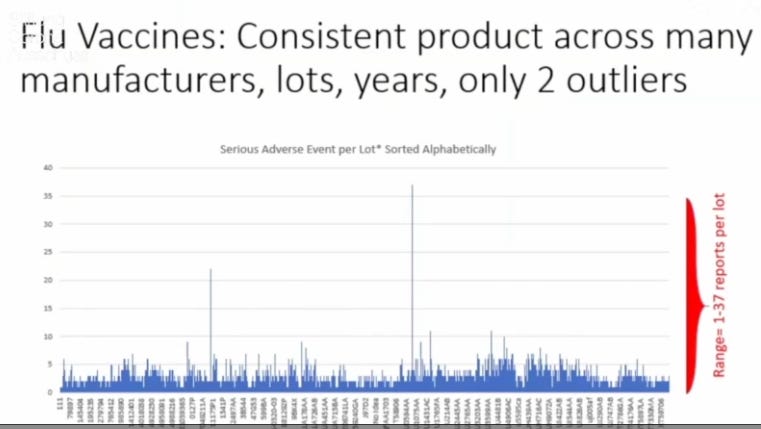
Note that Yeadon's interpretation of the COVID-19 quasi-vaccine batch/lot data differs from my own. It is perfectly possible that I am mistaken, but it is also possible that a man such as Yeadon who feels a world of anxiety coming out of the pharmaceutical industry is also looking for places to house that anxiety. But we do not need for the HLH to be true to recognize that there are more VAERS reports for these quasi-vaccines than for all vaccines in history despite the suppression of reporting. Whether the HLH is true or not does not change the total number of deaths or injuries attributable to the experimental products. And all of Yeadon's points about the nonsensical public policies strike me as well reasoned and valid.
At this point I'd like to offer a middleground hypothesis. It could very well be that a large part of the noisy AE batch distribution is due to points 1-4 that I made earlier. It could also be that there are a small number of toxic batches within all of that which resulted in additional harms.
Back to the Rappaport article. This discussion of bias among the "experts" responsible for investigating vaccine safety stands out as applicable to this moment.
A: The people doing the investigation are not really interested in looking at the facts. They assume that the vaccines are safe. So, when they do investigate, they invariably come up with exonerations of the vaccines. They say, “This vaccine is safe.” But what do they base those judgments on? They base them on definitions and ideas which automatically rule out a condemnation of the vaccine.
The interview gets extremely incendiary at this point:
Q: If vaccines actually do harm, why are they given?
A: First of all, there is no “if.” They do harm. It becomes a more difficult question to decide whether they do harm in those people who seem to show no harm. Then you are dealing with the kind of research which should be done, but isn’t. Researchers should be probing to discover a kind of map, or flow chart, which shows exactly what vaccines do in the body from the moment they enter. This research has not been done. As to why they are given, we could sit here for two days and discuss all the reasons. As you’ve said many times, at different layers of the system people have their motives. Money, fear of losing a job, the desire to win brownie points, prestige, awards, promotion, misguided idealism, unthinking habit, and so on. But, at the highest levels of the medical cartel, vaccines are a top priority because they cause a weakening of the immune system. I know that may be hard to accept, but it’s true. The medical cartel, at the highest level, is not out to help people, it is out to harm them, to weaken them. To kill them. At one point in my career, I had a long conversation with a man who occupied a high government position in an African nation. He told me that he was well aware of this. He told me that WHO is a front for these depopulation interests. There is an underground, shall we say, in Africa, made up of various officials who are earnestly trying to change the lot of the poor. This network of people knows what is going on. They know that vaccines have been used, and are being used, to destroy their countries, to make them ripe for takeover by globalist powers. I have had the opportunity to speak with several of these people from this network.
There are further moments in the interview that feel eerily prescient with respect to the current circumstances. It is worth reading every word, then thinking back on what we know about the history of the pharmaceutical industry and public health.
Lastly, remember that I was elevating the conversation about the real risks of these experimental quasi-vaccines before it was cool. I have learned a great deal more since and would only encourage every RTE reader to do what they can to take responsibility for their own health and the well-being of their families.

"A: The people doing the investigation are not really interested in looking at the facts. They assume that the vaccines are safe. So, when they do investigate, they invariably come up with exonerations of the vaccines. They say, “This vaccine is safe.” But what do they base those judgments on? They base them on definitions and ideas which automatically rule out a condemnation of the vaccine."
Vaccines are the sacred cow of medicine and the pharmaceutical industry. It's unthinkable to even consider that vaccines may not be safe. Anything bad that happens shortly after a vaccine has been administered is just a coincidence and surely not due to the vaccine.
I have personally not made up my mind on vaccines as a whole, but I stopped getting flu shots a year or 2 before covid (after being raised on yearly shots) and I knew as soon as there were talks of a covid vaccine that I would not take it. When you see the religious zeal with which mainstream doctors defend vaccines, I think you have to consider the possibility that vaccine science is not nearly as settled as its portrayed to be, because religious zeal doesn't lead to optimal research - even if you don't want to go into the more sinister aspects, such as believing the "medical cartel wants to kill you", as the researcher in the interview put it.
I've had the following argument used in a discussion on the Covid vaxx "If someone has an adverse effect shortly after getting the vaccine, attributing it to the vaccine is the same as saying someone who drops dead soon after drinking a glass of water, died because of drinking water."
No, I'm not making this up. They really do believe vaccines are as safe as water.
That section of the interview you posted is so dark that I find it difficult to even really comprehend. I don't want to believe it. But the evidence does seem to point in one direction only. I'm finding that the more I look into the "public health" apparatus, the more concerned I am.