


Defining Away Vaccine Safety Signals 10: DMED Revision, Low Resolution
The Vaccine Wars Part XLV

This DMED data story (articles here) of the heavily altered 2016-2019 data (and likely 2020) is one of the most important and undercovered stories of the pandemic. After 23 weeks, I still haven't seen anything like a good explanation for the substantial alteration of the historical data aside from sculpting the data to make the 2021 (the vaccination year) not look so bad.
Tonight Nick Kottenstette messages me after writing an article about the DMED data. His approach isn't quite correct, and I plan to work with him, but the exercise made me realize that I'd left an obvious analysis unperformed. When I stumbled on what happened with the data, it was because I was looking for reference data/rates of illness, which seems to be the same motivation for much of Nick's examination. While reading his article, it occurred to me to create an apples-to-apples comparison of 2021 diagnostic category summary data to the first published data for the years 2016-2019 (leaving out 2020 because that data was never published before the change in the reference data, which I believe was for 2016-2020, the first five years of data after the changeover to the ICD-10 medical billing code system).
Original Data Comparisons per Major Diagnostic Category
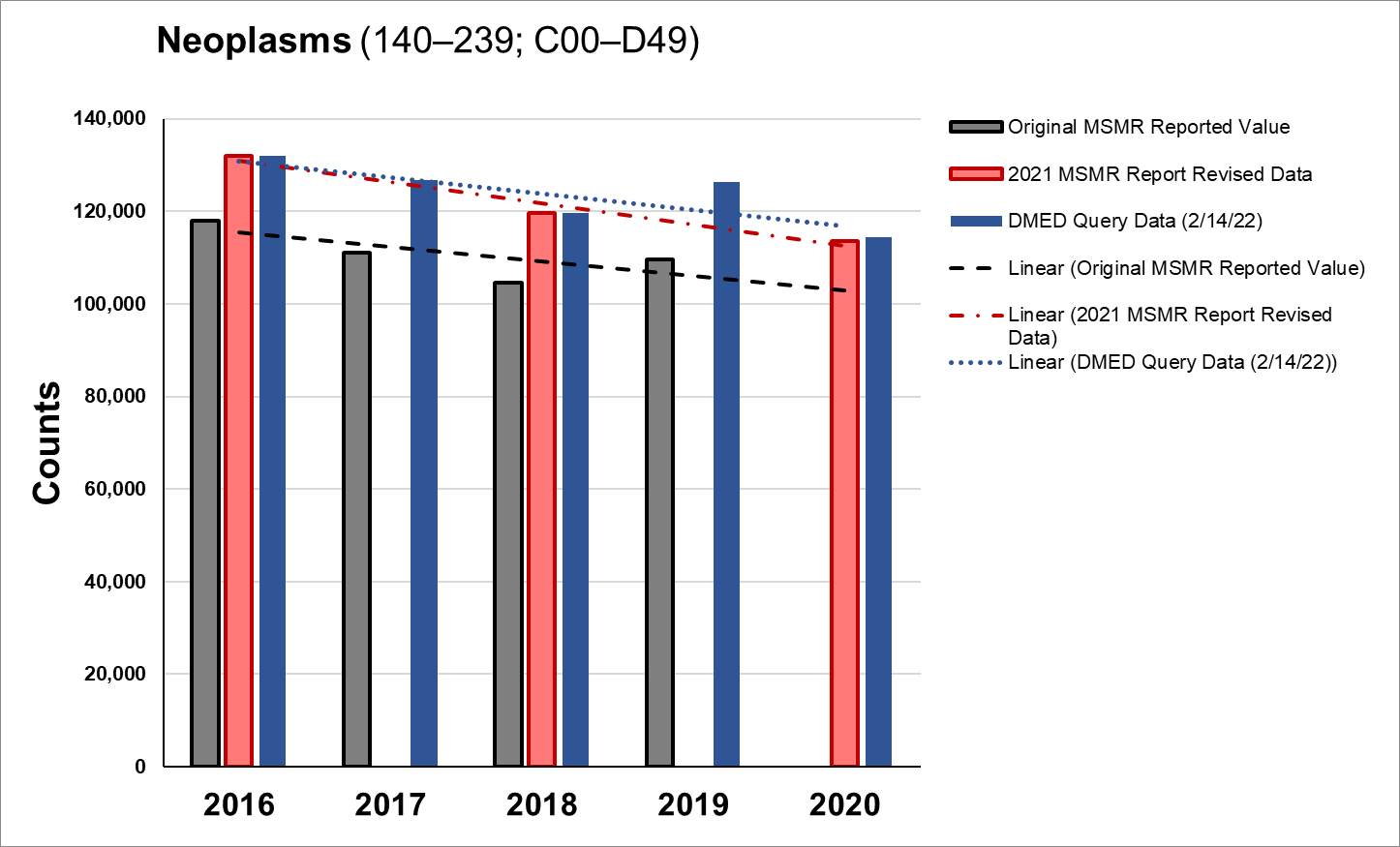
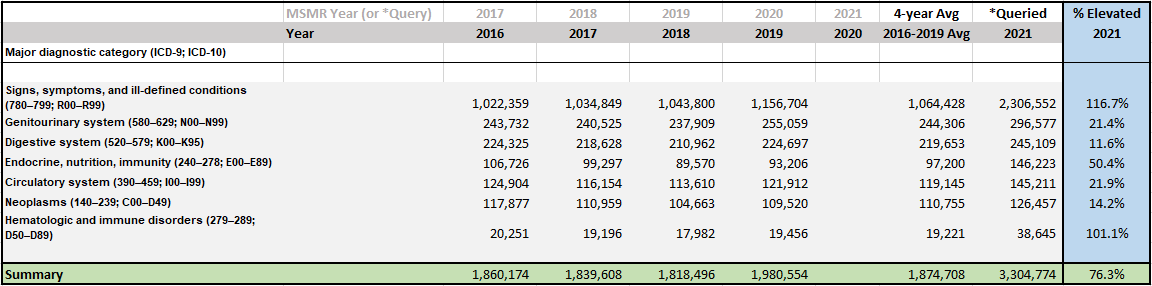
Note: Validation for this analysis is based on the fact that the mid-February 2022 queries from the DMED for all the major diagnostic categories (aside from the R-codes, ahem) matched the most recent data reported in the Medical Surveillance Monthly Reports (MSMRs). Graphically speaking, the red bars match the blue bars:
I went back to the pool of queries run for the major diagnostic categories to see where I could compare the queried 2021 data to the first-published MSMR snapshots for each of the years 2016-2019.
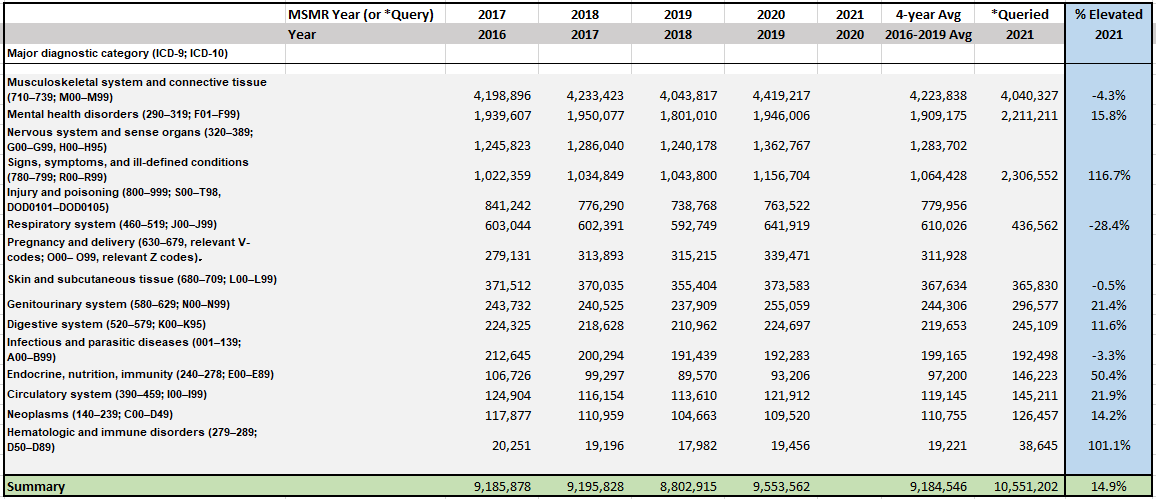
Note: I left out the Other category with the greatest number of ambulatory reports due to the fact that the definition of that category has not remained consistent over the years. I also did not have 2021 queries for the full data for H-codes, so I won't be able to evaluate the "Nervous system and sense organs" category (G00-G99; H00-H95), and similarly for the "Injury and poisoning" category (S00-S99;T00-T98). The "Pregnancy and delivery" category includes "relevant Z-codes", and though I could try to track down the definition, that complete data is not queried for 2021.
But this is plenty of data to work with. Note that the "Summary" data at the bottom only sums those rows for which we have the 2021 data. What do we see from the remaining 12 categorical diagnostic groupings?
Before we get started, recall that from 2012 through 2018, ambulatory health reports were on the decline throughout the military. That's what happens when troop participation in warfare scales down.
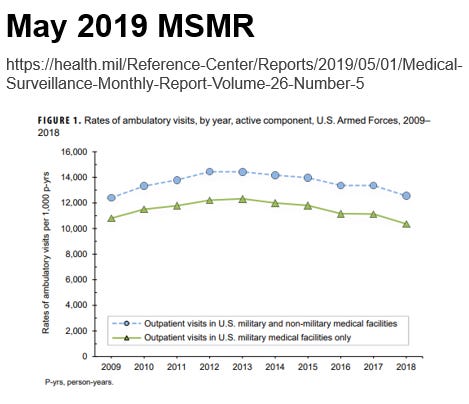
So, without a pandemic, I might expect overall totals for 2021 to be roughly 2-8% lower than the 2016-2019 average, though some categories are more stable than others.
M-Codes. We see a slight reduction (4.3%) in ambulatory reports for the musculoskeletal system and connective tissues category. This is not a category where we would expect either COVID-19 or the quasi-vaccines to have a major impact.
F-Codes. We see a 15.8% leap in mental health disorders. It could be argued that such an increase is due to the stress of being in a pandemic, or having a Commander in Chief who can no longer form a sentence or read one off a teleprompter.
R-Codes. Holy moly! The 116.7% increase in ambulatory reports for "Signs, symptoms, and ill-defined conditions and inconclusive laboratory reports" stands out. This "we have no idea what's wrong" category stands out as the one that would be the most associated with quasi-vaccine induced injury/illness.
J-Codes. It might seem strange that respiratory system illnesses declined so much (28.4%), but in actuality this drop seems to have begun in 2020 and continued into 2021 despite the emergence of COVID-19 in 2020 and a substantially increase in cases in 2021.
L-Codes. Illnesses associated with the skin and subcutaneous tissue saw a tiny decline. See 1 above.
N-Codes. Illness and injury of the genitourinary system rose a substantial 21.4%. This is where we should begin to worry about fertility, which is a systematic risk of the entire human population. Such risk should never be taken—particularly for a young and healthy population.
K-Codes. Illnesses of the digestive system went up 11.6%. This is where some cytokine-related inflammation might take place, spurred on by spike protein.
A/B-Codes. Infectious and parasitic diseases went down slightly (3.3%), and these should be largely unrelated to COVID-19 or the vaccines. However, we might expect this decline to mimic the decline in other respiratory illnesses if lack of deployment led to lower incidence. We might wonder if the quasi-vaccines lowered immunities.
E-Codes. The E-codes include immune disorders, and the ambulatory reports grew a whopping 50.4%. This is a startling signal of vaccine-induced injury and illness. I wish I could zoom in to every ICD-10 at once to isolate the immune disorders specifically.
I-Codes. Illnesses of the circulatory system grew 21.9%. There will be those who argue that this could be due to COVID-19 cases, but those people will have to answer why it is that COVID-19 cases were both more numerous and more severe in the military in 2021 than in 2020.
C-Codes and Some D-Codes. Neoplasms (cancer) were up 14.2% during the year of mass vaccination of the military. These vaccines may be associated with several thousand additional cases of cancer in the military. Such an increase, mapped to the population of the U.S., corresponds to a quarter of a million additional cases of cancer.
Other D-Codes. Blood and immune disorders should be at the top of our list of places to watch for vaccine safety signals, and we see these skyrocket 101.1% in 2021 relative to the recent four-year period.
Is somebody going to explain to me why this story isn't getting better traction?
Summary
If we remove the four categories with lower 2021 numbers, which do not seem to be particularly related to vaccination, we see a dramatic 45.8% rise in ambulatory reports among the remaining eight diagnostic categories.
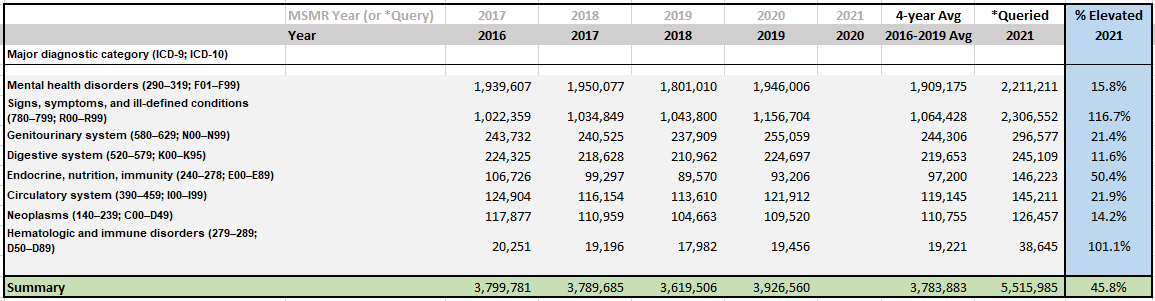
Further, if we remove the mental health disorders, which seem least likely to be associated with the quasi-vaccines, we see an explosive 76.3% rise in ambulatory reports among the remaining seven diagnostic categories. These are primarily illnesses of the blood, immune system, the digestive system, cancer, and cases of illness that physicians haven't figured out. On face, this makes the vaccines look like a total disaster.
I do wish that I had complete data for pregnancies and other fertility information as I know that many people are worried about the quickly dropping birth rates across numerous reporting nations. Had I not had to take so much time out to push this story myself, correct the propagation of misinformation, and try to get wheels moving toward investigation and accountability, I would have had more time left to direct the data mining process. But here we are.
Special thanks to paid subscribers during these past few months when I've spent a few hundred hours on this project. Your support is always appreciated. All pandemic analysis related to understanding medicine and health will always continue to remain free for all to read.
Fantastic analysis. Sincerely thank you for everything that you are doing. We are praying for your protection, good health, help, healing, and for love and light to shine so brightly that people can no longer keep their eyes closed and ignore the data. Truth is and will prevail. God speed.
Yes, seems you have stumbled across a major story here. The core allegation that the DOD retrospectively revised medical report data upwards for the years prior to the vax rollouts, to conceal an anomalous increase after the rollout, needs reiterated in as simple a form as possible to maximize chances of the story gaining traction.
The bureaucratic explanation of correcting an innocent database sync error (or whatever) isn't credible when we consider the differential rates of adjustment by category of illness. It would be interesting to "steel man" that explanation and say, OK, what kind of innocuous technical error could _possibly_ result in that sort of differential under-reporting by category.
The sad truth is that the government, especially the DoD, monkeying around with data and secrecy has been "tuned out" in the MSM since the Snowden revelations. Overlay the vax omerta on top and you've got abnormally large barriers to acknowledgement.